Welcome to the /r/tretinoin wiki!
I was just prescribed tretinoin, what should I know?
PM Step 2) - Apply tret and moisturizers
Buffering option 1 (The Sandwich method):
Buffering option 2 (The Moisture Blanket method):
No buffering option (The Rogue method):
AM Step 3) - Apply Moisturizer and SPF
Common Questions and Discussion Topics
If I stop using tret will I purge again if I restart it?
How do I avoid flaking and peeling?
Which formulation should I use?
Still lots of irritation after 2-5 months?
Tretinoin vs Adapalene vs Tazarotene vs Retinol vs ...
What is tretinoin NOT as good for?
Does tretinoin thin the skin or thicken it?
Is Adapalene good for anti-aging?
[1] There is no evidence that sun sensitivity returns to normal after continual usage of tretinoin.
[2] There is some evidence that higher strengths of tretinoin is more effective for acne.
[4] Using a moisturizer improves tolerability for tretinoin.
[5] Moisturizer improves tolerability for tazarotene and does not negatively impact efficacy.
[7] Gentle cleansers and moisturizers are key to treating acne.
[9] Using a moisturizer with ceramides makes tretinoin hurt less.
[6] The increased cell turnover triggered by tretinoin does not “use up” your cells early.
Quickstart
I was just prescribed tretinoin, what should I know?
- YOU MUST USE SUNSCREEN. This is non-negotiable.
- Yes, even if you have dark skin.
- Yes, even though you likely use tret at night.
- If you can’t commit to wearing sunscreen daily, tretinoin is not right for you.
- NO WAXING. Do not wax while using tretinoin, your skin will rip off. Shared with permission by /u/Nice_Turtle_1
- Shaving, threading, and epilating are ok forms of hair removal.

- Expect to see irritation within 2-3 weeks, and improvement within 4-6 months of starting tretinoin.
- Hydration is key. Use moisturizer both morning and night.
- Start slow! The effects won't kick in for the first several weeks.
- START SLOW - 2x a week at first, slowly increasing in frequency based on how your skin feels. A tentative schedule might be 2x/week for 2 weeks, 3x/week for 3 weeks, etc. Don't stick to a schedule if you’re getting extreme irritation. If moisturizer or cleanser stings very badly, take days off to recuperate and mend your skin.
- Some derms tell you to start every night. This is almost always a mistake.
- A basic routine is best. Cleanse 1x a day with a gentle cleanser, moisturize twice a day, and apply sunscreen every morning. See below for more routine tips.
- Start gentle! When you're first using tret, stop all other actives: no BHA, AHA, or other harsh products like benzoyl peroxide or azelaic acid. Vitamin C works for some and not others (you’re the expert on your skin and will have to decide what works for you).
- This means no other actives at all. Morning AND night.
- Stop other actives at least one week before starting tretinoin.
- If your derm prescribed more, then it's up to you if you want to follow their advice. You have to find the balance between listening to your skin and following your doctor’s orders. We strongly recommend going slow and being very gentle. (Once you've been using tretinoin for 6+ months, you can add these back in as needed).
Further reading:
- A very thorough post about how to use retinoids the right way from skinacea.
- A bunch of personal reviews and tips from people over at /r/skincareaddiction.
- Advice from a dermatologist about how to use tret. And a little more discussion.
- Do you have other troubleshooting tips? Message the moderators about contributing to the wiki!
Routine Suggestions
PM Step 1) - Cleanse
- Wash/Cleanse your face with a gentle cleanser and cool water to remove makeup, sunscreen, etc. Gentle cleansers are key. If your face feels 'tight' after using your cleanser it is too harsh, get another one.
- Popular cleansers: Cetaphil, CeraVe Hydrating, Vanicream Gentle Hydrating, CeraVe Foaming (tends to be more drying than the Hydrating one). Lots more recs at /r/skincareaddiction.
PM Step 2) - Apply tret and moisturizers
Short contact therapy (the most gentle method):
- Apply tretinoin to your dry, clean skin.
- After ~5-10 minutes, rinse it off.
- Immediately apply moisturizer.
- Slowly increase the amount of time you leave the tretinoin on your face, going up by ~5 minutes every week until your skin is accustomed to it.
Buffering option 1 (The Sandwich method):
- Moisturizer on damp skin after cleansing in step 1 above. Research even shows that moisturizers even enhance the effects [4], [5], [7], [9], especially a moisturizer containing niacinamide [8]. Light serums are less good because they increase absorption and therefore increase irritation.
- Wait for skin to dry
- Apply tret
- More moisturizer, then occlusive (optional) > Bed
Buffering option 2 (The Moisture Blanket method):
- Wait for skin to dry after step 1 cleanse above.
- Apply tret to completely dry skin.
- Wait for tretinoin to dry (~5 mins)
- Apply moisturizer, then occlusive (optional) > Bed
- NOTE: see this comment for an extensive discussion around occlusives layered over tretinoin. TL;DR: tretinoin products are designed with normal “trans-epidermal water loss” taken into account. Adding an occlusive on top disrupts the expected water loss, and could cause increased irritation. Always patch test any changes!!
No buffering option (The Rogue method):
- Wait until your skin is totally, completely dry after cleansing in step 1 above.
- Apply tret > Bed.
AM Step 3) - Apply Moisturizer and SPF
- Wake up
- Splash your face with cool water, gently rub with your hands. There is no need to use a cleanser in the morning, and it can dry you out even more. Water is enough for most people! (You are the expert on your skin, though, so do what works for you).
- Apply moisturizer. Research even shows that moisturizers even enhance the effects [4], [5], [7], [9], especially a moisturizer containing niacinamide [8].
- Wait for the moisturizer to dry.
- Apply sunscreen. You should be using a minimum of SPF 50, with PA ++++. More info about sunscreen below.
General routine tips
Wear sunscreen. Sunscreen is an absolute must while using tretinoin. If you cannot commit to daily use, find another ingredient to use. Azelaic acid is excellent.
Always apply retinoids to dry skin. That means either 1) pat-dry your skin after cleansing and wait a few minutes for it to dry completely, or 2) wait for your moisturizer to dry completely. It has long been known that hydration of the stratum corneum increases its permeability[11, 12, 13, 14]. Hydration increases skin permeability overall [11, 12, 14], and also increases the absorption of topically-applied molecules [13]. Additionally, manufacturers advise using topical drugs on clean and dry skin, so that’s what you should do. If your skin is wet at all when you apply tretinoin, you will likely see an increase in flaking, peeling, and irritation.
Apply a pea-sized amount of tretinoin for your entire face. Apply a small dot in the center of forehead, on cheeks, nose, and chin. Sweep out to outer parts of the face to spread it. Do not put directly under eyes, around the mouth or in the nose folds. It may feel as if it is not enough, but it is. The reason for this is because tretinoin being a fat soluble molecule is immediately absorbed by our cells and bound to its receptors. When all of the receptors become saturated, the excess is stored in the cell, and the amount of unused tret in our skin is exactly what has the strongest link to irritation and side effects. So if you’re using more than it’s necessary every time, the amount of free tretinoin in your skin will quickly skyrocket. The best way to check if you’re using more than you should is to gently apply a thin tissue to your face when you finish spreading your tret. The tissue should fall off. If it sticks, you’ve used too much.
Only apply tretinoin at night. It degrades in the sunlight, so there is no point in wearing it during the day.
Apply tretinoin evenly to your entire face. Tret is NOT a spot treatment. Uneven application can mean weird patches of irritation and discoloration, especially on darker skin tones.
Buffering does not decrease effectiveness. For acne treatment, studies show buffering does not cause problems with tazarotene, a relative of tret. We haven't seen any studies of buffering with tretinoin (Message the moderators if you have research you’d like to share!). Some people in the sub say buffering doesn't work as well, especially with the micro-gel forms. Redness and flaking are not desirable side-effects, minimizing them will not decrease effectiveness. If you don’t have irritation, it doesn’t mean tretinoin isn’t working. It can take 1-3 weeks to feel the effects.
Use moisturizer! Keeping skin healthy and happy is key to treating acne. Research shows that using moisturizer actually ENHANCES the effects of retinoids[4], [5], [7], [9], especially a moisturizer containing niacinamide [8]. An occlusive like Vaseline or Aquaphor applied on top of moisturizer at night can minimize Trans-Epidermal Water Loss and keep skin moisturized and healthy without clogging pores.
- Examples of good moisturizers: Cerave in the Tub moisturizer, Vanicream Lite moisturizer, Cetaphil.
Required: Sunscreen
Sunscreen is *required* when on any retinoid. Not using sunscreen leaves your skin extremely vulnerable to sun damage and does more long-term damage than short-term good.
Dark-skinned folks also need to wear sunscreen.
**If you cannot commit to using sunscreen daily, do not start tretinoin.** Tretinoin makes you sun sensitive for up to 2 weeks [citation needed] so wear sunscreen for up to 2 weeks after stopping tret. There is no evidence that sun sensitivity returns to normal with long-term use of tretinoin.[1]
- With tret, you need a minimum of SPF 50, PA++++ (UVA protection). Quick reminder that UVA rays cause tanning, hyperpigmented sunspots, and ultimately fine lines and wrinkles. UVB causes sunburn. Both can cause skin cancer.
- The "SPF" rating only rates UVB protection, not UVA protection. In the world of /r/AsianBeauty, UVA protection is rated by PPD (persistent pigment darkening) or the PA system, which classifies PPD levels in a product. Read more about PPD here.
- You always need to apply enough of your sunscreen! When sunscreens are tested for SPF labels, it is always applied at a density of 2 mg/cm squared. The mentioned quantity is needed for sunscreen to form a uniform film on our skin, which is crucial for optimal protection. In reality that translates to about 0.9-1,4 grams of product you need to use every time, for face only. The usual tool of measurement people use so they don’t bother with numbers are ‘fingers’ of sunscreen. For most people, 2 full length fingers of sunscreen (just like this) are enough for face only, and 3 fingers for face, neck, and ears. This method is not perfect because the amount of product that ends up on your fingers significantly varies from product to product, depending on vehicle, thickness, etc. That’s why it would be wise to measure approximately how much product you need, and measure it for every sunscreen you use, because it will vary. There are number of ways to do that:
1) Use teaspoons to measure. About ¼ to ⅓ of a teaspoon would be the amount needed. This is again flawed because you can only measure approximately.
2) Measure the estimated surface area of your face using this method. It should be around 400-500 cm squared, and you can add 10-20% to that taking into account our face is actually a 3D model. Then multiply that by 2 and you’d have the estimated amount of sunscreen you need to apply to your face in milligrams. Get a small 2ml syringe, and use it to measure exactly how much sunscreen you’d need (if we estimate that 1g = 1ml). Now use the syringe to dispense the sunscreen to your palms, or your fingers, so you can get the feeling of how much you should be using each subsequent time.
3) After measuring out your face, measure out the correct amount on a digital scale that measures in milligrams, if you happen to have one.
We just want to note that this is not required for optimal protection, but it is super helpful for preventing you from under or over-applying your sunscreen. - It is recommended that you reapply sunscreen at least every two hours, and always after showering, swimming, heavy sweating etc. This is because the uniform film that is needed for the sunscreen to properly work breaks down in that period and it needs to be formed again, regardless of if you were exposed to sunlight in that period or not.
- Windows do not block UVA rays, but the amount of UVA rays that reach you indoors depends on many variables. Here is a very useful video by Lab Muffin explaining the situation and we suggest you see it and decide for yourself if and when you need to wear your sunscreen indoors. We would like to note that it is still better to wear sunscreen when you don’t need to than accidentally not wearing it when you do need it, so the best practice is still putting on sunscreen every single day regardless of what you’re planning to do that day.
- Here is an excellent comparison of favorite AB sunscreens.
- Sunscreen does not need to sink in to work: both mineral and chemical sunscreens form a film on the skin which mainly absorbs UV rays and prevents sun from causing damage.
- Sunscreen filters have improved a lot in recent years, but the FDA in the US has not yet approved them. They are totally safe and effective, the FDA is just slow. Look at Japanese or Korean sunscreens for the latest in cosmetically elegant, light, non-sticky, instantly drying, non-greasy sunscreens!
- See the latest HG list for sunscreen from /r/skincareaddiction for lots of sunscreen recommendations!
- The best sunscreen is one you'll use. If you have an SPF 30 sunscreen you love, use that!!
Further reading:
- A great post from labmuffin on “How Does Sunscreen Work?”
- An incredibly detailed comment from the amazing /u/Feather-Light about different sunscreen filters and their effectiveness.
- A great post from Kind of Stephen on why Avobenzone is safe and effective, but can still sting your eyes.
- More info about the difference between chemical and physical sunscreens.
- A research thread showing no evidence for the claim that skin's sun sensitivity levels return to normal after using tretinoin for a period of time.
Common Questions and Discussion Topics
All about purging
What is purging?
(Thanks to /u/caffeinatedlackey and /u/condescending-fork for their great contributions to this section!)
To understand purging you need to first understand the skin cycle. The ELI5 version is that the organ generates new cells from the inside out to replace older cells that slough off. This is called turnover. For adults the cycle is roughly 6 weeks.
When you're a child, your skin generates new cells more quickly, which is one major reason why kids are blessed with great skin and heal more quickly from injuries.
Retinoids accelerate the skin cycle, meaning that you generate new cells more quickly and your skin has an enhanced ability to heal. However, this also means that the acne cycle (impurities and bacteria underneath your skin coming to the surface as acne) accelerates as well. Typically, it may take a few weeks for the acne lesion that is formed in your skin to make its way to the surface and show up to your skin. So, purging is actually a phenomenon by which acne lesions that were already formed in your skin make their way to the top of your skin faster than they usually would, giving the impression that you’re getting new acne, when you’re actually just getting rid of ‘old’ ones faster. If purging is bound to happen to you, it cannot be avoided, nor should you want to avoid it, because you’re basically just dealing with your existing problems faster.
By the nature of its physiology, purging will usually last only for 6-8 weeks and will usually appear only on your usual breakout locations. If you’re getting new waves of acne in places you usually didn’t have them, or if those acne linger, or just keep coming again and again, that is likely not a purge. A purge is, by its definition, a one time thing. There is no ‘purging for 6 months’ or ‘second, third, sixth etc wave of purging’. That would likely be a consequence of irritation.
This does not mean that tretinoin will bear its full effects in 6-8 weeks, you can still get acne after that period like you used to, but it would most likely not be considered a purge. However, once tret shows its full effects after about 6 months, and your skin’s structure gets in order, it is important to keep maintenance of those effects and continue using tret. After that some people never have any acne again, and others have a reduced amount. It's all individual.
Does everyone purge?
Purging is also actually not that common, people are just usually misinterpreting it. Here is a link to one study to support that, and the study defined purging as a 10 to 20% increase in inflammatory lesions, which is a significant but not an enormous difference[10].
Remember, irritation also causes breakouts. Retinoids are very irritating. THE SLOWER YOU GO, THE LESS LIKELY YOU ARE TO HAVE IRRITATION. Go as slowly as possible and focus on hydration and gentleness.
If you don't have regular acne you are less likely to purge. Closed comedones may purge by becoming pimples.
What does a purge look like?
A purge should not be more than a 20% increase in breakouts. Closed comedones often come to the surface, so it can feel like your skin is getting much worse.
How long does the purge last?
It can last anywhere from a few days to 6-8 weeks. The purge should only be a 10-12% increase in your existing acne [10]. If your purge is worse than that, or lasts longer than 6-8 weeks, it is probably not a purge and is irritation instead. You may be sensitive to an ingredient in your tretinoin formula, but far more likely - you’re using it too much, too often. You can check up with your dermatologist to discuss what’s your best plan, changing the formulation or changing the regimen.
If I stop using tret will I purge again if I discontinue, and then restart it?
Maybe! This is difficult to predict.
All about flaking / peeling
How do I avoid flaking and peeling?
- Make sure your skin is completely dry when you apply tretinoin.
- A good moisturizer is key. Using a moisturizer actually improves tret outcomes[4], [5], [7], [9] especially a moisturizer with niacinamide [8]. Vanicream Lite, and Cerave are popular options.
- Vaseline or Aquaphor used on your tret ‘off’ nights can also really help prevent dryness. Pat on a very thin layer gently - don't slather it, just apply a thin layer.
- Oil cleansing can work for many as a way to gently remove the excess skin. Get an emulsifying oil cleanser that will wash off easily.
- Consider skipping a night of tret if you have lots of peeling. Yes that may slow down your progress by a few days but a damaged moisture barrier can take months to recover. Go slow. Skincare is a marathon.
- Make sure your routine is hydrating enough. Hydrating toners like those from Hada Labo can really help (Premium is the most popular since it has urea and 5 sizes of hyaluronic acid and is incredibly hydrating). /r/asianbeauty has lots of recs.
All about buffering
- Buffering does not impede function, and in fact using a moisturizer actually improves tret outcomes[4], [5], [7], [9] especially a moisturizer with niacinamide [8]. This is partly because it minimizes the irritating side-effects and makes people better able to tolerate more applications of tretinoin.
- Having a healthy skin barrier is important to acne treatment. Everyone can benefit from a moisturizer (yes even if you have oily skin). Keep your skin moisturized and healthy to prevent breakouts and heal faster when you do break out.
Which formulation should I use?
Tretinoin is available in 3 primary vehicles: cream, gel, and gel microsphere. The cream is often preferred by those who have drier skin. The gel is good, although it does have alcohol but a solid routine can make up for it. The microsphere formulation really helps with irritation and the texture is gel-cream like, but it may be less effective when buffering for some, so if you have extremely dry skin it may not work as well. (Thanks to /u/rose_valley for contributing to this section!). The micro form may also be much more photostable than the other two options. The “vehicle” in either formulation can trigger breakouts - so if you’re still breaking out after 4-6 months, consider switching types (gel → cream, cream → gel).
What percentage should I use?
- for anti-aging: A comparison between 0.025% and 0.1% shows similar improvement, but much less irritation for the lower percentage [citation coming].
- Another study showed that 0.05% shows improvement over 6 months compared w/ 0.01%. It's possible over many years the lower percentage would catch up to the higher percentage. Here is a picture of reasonable results to expect after 9 months on 51-year-old skin.
- for acne treatment: the lowest percentage that works is best. Higher percentages cause more irritation, and increased irritation causes acne.
Troubleshooting
Still lots of irritation after 5 months?
If you're still getting tons of irritation, there are a few common issues we've seen. As with all skincare, your mileage may vary! Some have success doing everything "wrong". This is just a troubleshooting guide, not rules set in stone. Contact your doctor if you're very concerned! Here are some ideas:
- Did you jump into a really high percentage? Consider scaling back. 0.05% is pretty high at first. 0.1% is VERY high. It can help to start with 0.025% or 0.04%. The micro formulation is generally less irritating.
- Switch formulations. Some people experience breakouts triggered by a particular formulation. If you’re still breaking out after 4-6 months, consider switching types (gel → cream, cream → gel).
- Is your routine too irritating? Cut out ALL other actives and focus on hydration.
- Are you using it too *infrequently*? The skin has to go through the retinization process. That inherently involves some irritation. If you go too slow, your skin may actually never acclimate [citation needed - I've seen it just need to find it again...]. If you're only using tret a few times a week, try INCREASING your usage. At least 4x a week.
- Are you moisturizing enough? All skin needs moisture and hydration: check out the tips and links above for lots of info on a good routine.
Do you have other troubleshooting tips? Message the moderators about contributing to the wiki!
What is tretinoin?
- A wonderful info page on retinoids was put together by the superhero mods over at /r/skincareaddiction.
- Info on what tret is and how to use it properly from labmuffin.
- Selections from Leslie Baumann's Cosmetic Dermatology shared by the generous and kind /u/S3mirmis.
Tretinoin vs Adapalene vs Tazarotene vs Retinol vs ...
Look here for a chart comparing the different types of retinoids.
- Tretinoin binds to RAR alpha, beta, and gamma receptors
- Tazarotene binds to RAR beta and gamma receptors
- Adapalene binds to RAR beta and gamma receptors, but less effectively than Tazarotene (FYI this is the reason why this ingredient is FDA approved for acne, but not anti-aging)
(Thanks to /u/jdm71384 for this succinct write-up!)
Tretinoin vs Adapalene vs Tazarotene vs Retinol
(Thanks to /u/rose_valley and u/healingfemme for contributing to this section!)
While all of them are derivatives of Vitamin A, Tazarotene is the strongest form of topical vitamin A [30]. Retinoids are fat soluble compounds, and as such, they are freely and immediately absorbed into our cells upon application, where their receptors, Retinoic Acid Receptors (RAR) alpha, beta, and gamma, can be found. Tretinoin and adapalene, being a form of retinoic acid, can instantly bind to those receptors, but retinol and retinal can not and they need to be converted to retinoic acid first. Retinol converts to retinal, and retinal converts to retinoic acid. For that reason, retinol is much better tolerated, but its effects are also more limited. Because those receptors work by modifying gene expression, all positive effects of tretinoin and adapalene can not be immediate and take time, which is even longer for retinol due to the extra steps necessary [30].
What is tretinoin good for?
- Treating acne
- Anti-aging (tretinoin is considered the gold standard for anti-aging treatments).
- photodamage (fine wrinkling around the eyes, crease lines around the mouth and cheeks, yellowish skin, telangiectasia over cheeks, periorbital comedones, wrinkling of skin and the backs of the hands, and solar keratosis.)
- PIH (brown-ish hyperpigmentation).
What is tretinoin NOT as good for?
- minimizing redness (increased vascularity means redness can actually INCREASE for some).
- minimizing irritation (tretinoin is one of the most irritating ingredients).
- PIE. Post-irritation erythema. Erythema is dilation of the blood vessels. Tretinoin increases vascularity -- creates more blood vessels -- so it can make erythema worse. If you have pale skin, this looks like redness. If you have darker skin, this can look like a “glow”. If you’re pale, azelaic acid, niacinamide, vitamin c are better for dealing with hyperpigmentation.
Does tretinoin thin the skin or thicken it?
One study found that the stratum corneum (outermost layer of skin) "became compact in the first 3 to 6 months whereas it returned to normal (basket weave pattern) in 12–24 months and remained normal until the end of the therapy" (source, arg I had it then lost it, once I find it again I’ll add it here.), which sounds like the thinning of the stratum corneum goes back to normal with continued use. This does NOT mean sun sensitivity goes back to normal [1].
Is Adapalene good for anti-aging?
Inconclusive! Read more here.
Where can I get tretinoin?
- Search for a reputable dermatologist in your area.
- Sign up for an online dermatology service like Curology, Apostrophe, or PocketDerm (the names are changing all the time). Here’s an old discussion about Curology.
- Americans can order tretinoin online from a wide variety of places.
- Here are specific instructions for ordering online,
- In some countries tret is available over the counter.
- Some further information about ordering online.
Is tret photostable?
- Micro gel vs gel formulation: One study found a degradation of 11% after an 8-hr exposure to flourescent light vs a degradation of 86% after 2 hours exposure to fluorescent light for the gel version [citation coming].
- Notes: no studies have been done that compare the cream and gel formulations. Also, both authors of that study reported conflicts of interest with the company that makes the micro version, so they do have a slight reason for bias towards pushing the microionised form. Take that as you will.
Long-term use
- Tret is safe to use long-term. Here is a picture of reasonable results to expect after 9 months on 51-year-old skin.
- It is possibly not safe to use while breast-feeding or while pregnant. Isotretinoin (accutane) causes birth defects, so with an abundance of caution medical providers recommend avoiding tretinoin too. But there have been no studies either way (and there probably will never be: it's too risky to study pregnant women).
Use while pregnant or trying to conceive
For more information about using Tretinoin during pregnancy or while breastfeeding see: https://mothertobaby.org/fact-sheets/tretinoin-retin-a-pregnancy/
Before and Afters
This gallery contains some inspiring before and after pictures from /r/tretinoin members
From /u/LongJourneySadly

From /u/ewhelann
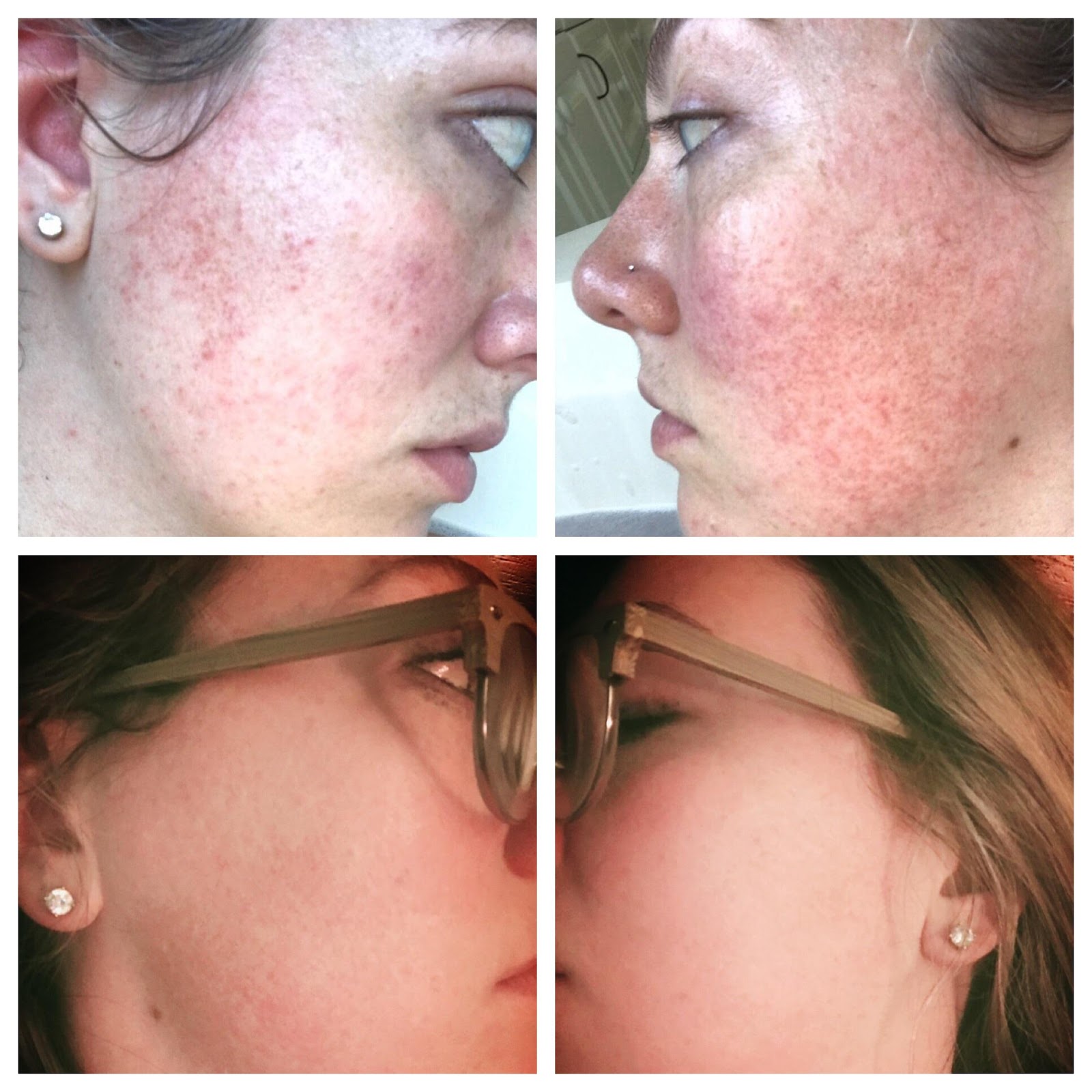
From /u/alex0332:

From /u/zScourgez:

{kind=link}
{kind=link}
(We got permission to post all of these pictures, but if any of these pictures are yours and you have changed your mind and you would now like us to remove them, please message the moderators with proof they’re you so we can take them down!)
Research Summaries
Have you read other research papers you’d like to add here? Message the moderators so we can add them to the wiki :)
Sun sensitivity
[1] There is no evidence that sun sensitivity returns to normal after continual usage of tretinoin (while using tretinoin).
Wear sunscreen daily, and reapply after 2 hours of cumulative sun exposure. So if you walk to your car in the morning and you're in the sun for 15 minutes, then sit in your office away from a window for 3 hours, that counts as 15 minutes of direct sun exposure and there's technically no need to reapply. HOWEVER, sweat and friction like rubbing your face also removes sunscreen. How much? There’s really no way to know, so this is why dermatologists just recommend the general rule of “every 2 hours”. If you sit near windows indoors, you also still need to use sunscreen since windows don't block UVA light.
If you discontinue tretinoin, your skin will eventually return to normal levels of sun sensitivity. The exact timeline is unknown - probably safe to assume that your skin will be normal a month after quitting. If you are concerned about aging, you need to wear sunscreen every day no matter what.
Acne
[2] There is some evidence that higher strengths of tretinoin is more effective for acne.
Title and authors: Safety and Efficacy of Tretin‐X Compared With Retin‐A in Patients With Mild‐to‐Severe Acne Vulgaris (2007). Webster Guy F. MD, PhD.
Variables: 3 concentrations of tretinoin from 2 brands (Tretin-X and Retin-A) and 2 formulations (gel vs cream)
Participants: 1642 adolescents and adults, 12–40 years of age, with mild‐to‐severe acne vulgaris
Methods: Four double‐blind, three‐treatment, parallel‐group studies randomly assigned 1642 adolescents and adults, 12–40 years of age, with mild‐to‐severe acne vulgaris to receive topical tretinoin therapy with Tretin‐X, Retin‐A, or placebo (drug vehicle) as 0.1% cream (study 1), 0.025% cream (study 2), 0.025% gel (study 3), and 0.01% gel (study 4) once daily for 84 days. The primary efficacy measures were overall acne severity and the number of inflammatory lesions. The secondary efficacy measure was the total number of lesions.
Results: In each trial, Tretin‐X and Retin‐A were clinically equivalent according to all primary and secondary end points at Weeks 2, 4, 8, and 12, a finding also demonstrated by the averaged scores from Weeks 2 through 12. Moreover, each active treatment was significantly more efficacious than placebo at the conclusion of the study ( p≤0.05). Both of the Tretin‐X and Retin‐A formulations compared in each study were well tolerated. The severity of erythema and peeling did not differ significantly among the three groups studied. Conclusions. The four bioequivalence studies demonstrated that Tretin‐X and Retin‐A tretinoin products behaved similarly in patients with mild‐to‐severe acne vulgaris and were thus clinically bioequivalent. Both treatments were well tolerated, and their associated adverse events were similar to those with placebo.
Conflicts of Interest: None
Notes: The real important results here are the comparison between the brands, comparison between gel vs cream, and the comparison between the strengths. The article is paywalled so I'll have to summarize, but the two brands were basically equivalent and so was the gel vs the cream. As for the concentrations, the metric they use in this study is the "percentage reduction in mean total number of acne lesions from baseline to week 12" and the numbers are around (not exact due to copyright) 44% for 0.01%, 55% for 0.025%, and 71% for 0.1%. So yes, there is likely evidence that higher strength of tret = better effectiveness for acne!
Major thanks to /u/CarlFriedrichGauss for this summary!
[3] Aloe vera topical gel enhances tretinoin efficacy compared to a placebo in a randomized, double-blind, prospective trial.
Title (Year). Authors: Effect of Aloe vera topical gel combined with tretinoin in treatment of mild and moderate acne vulgaris: a randomized, double-blind, prospective trial. (2014) Hajheydari, Zohreh; Saeedi, Majid; Morteza-Semnani, Katayoun; Soltani, Aida
Variables: Compare the efficacy and safety of the combination of tretinoin (TR) cream (0.05%) and Aloe vera topical gel (50%) with TR and vehicle.
Participants: 60 subjects with mild to moderate acne vulgaris
Methods: Randomized, double-blind, prospective 8-week trial evaluated inflammatory and non-inflammatory lesion scores and tolerability.
Results: The combination therapy showed superior efficacy to TR and placebo. TR/Aloe vera gel (AVG) was significantly more effective in reducing non-inflammatory (p = 0.001), inflammatory (p = 0.011) and total (p = 0.003) lesion scores than control group. The highest percentage of adverse cutaneous effect was reported for scaling. At the end of study, erythema in the TR/AVG-treated group was significantly less severe (p = 0.046).
Conflicts of Interest: None listed...
Notes: This is now the 3rd paper I've seen showing that using moisturizer actually *enhances* tretinoin effectiveness.
[4] Using a moisturizer improves tolerability for tretinoin.
Title (Year). Authors: Adjunctive use of a facial moisturizer SPF 30 containing ceramide precursor improves tolerability of topical tretinoin 0.05%: a randomized, investigator-blinded, split-face study. Schorr et al., 2012
Variables: This was a randomized, investigator/evaluator-blinded, split-face comparison in subjects with healthy skin.
Participants:
Methods: Subjects applied tretinoin cream 0.05% once daily to the whole face and Cetaphil Moisturizer (CM) once daily to one side of the face based on randomization. Tolerability, preference and skin hydration were evaluated at each week, and a cosmetic acceptability questionnaire regarding CM was completed at the end of the study.
Results: The majority (about 83% to 86%) of subjects experienced skin irritations on both sides of their face, though predominantly mild for the CDM + tretinoin treated side. Tolerability preferences favored the CDM+tretinoin sides.
Conflicts of Interest: None listed...
Notes: This was a great study. Love the evaluator-blinded study. Doesn't seem to say anything about efficacy, only tolerability.
[5] Moisturizer improves tolerability for tazarotene and does not negatively impact efficacy.
Major thanks to /u/scumteam14 for this writeup!
Title (Year). Authors: Moisturizer use enhances facial tolerability of tazarotene 0.1% cream without compromising efficacy in patients with acne vulgaris Tanghetti, Emil, et al. Poster presented at 32nd Annual Hawaii Dermatology Seminar. 2008.
Variables: once daily 0.1% tazarotene cream vs once daily 0.1% tazarotene cream + twice daily moisturizing cream (with the PM moisturizer being applied 20 minutes prior to tazarotene)
Participants: 96 participants with mild to moderate facial acne completed the study (originally 119); originally 39 in the tazarotene alone group and 80 in the tazarotene + moisturizer group
Methods: Multicenter, investigator-blind, randomized, parallel-group, 16-week study
Washout periods:
- 14 days for topicals (OTC & prescription)
- 30 days for antibiotics or corticosteroids (systemic presumably)
- 90 days for birth control (unless the pt. had already been using BC for at least 90 days, in which case they continued to use BC)
- 6 months for systemic retinoids
Routines:
All participants cleansed twice daily with a gentle cleanser
Both groups applied tazarotene in the PM. The tazarotene + moisturizer group applied moisturizer in the AM and PM, with the PM moisturizer being applied 20 minutes prior to tazarotene. The tazarotene-only group was allowed to use moisturizers, but only if absolutely necessary.
Both groups were encouraged to avoid UV exposure, and to use sunscreen if necessary.
Investigator ratings:
- inflammatory lesion count (papules & pustules)
- noninflammatory lesion count (open and closed comedones)
- overall disease severity (0=none to 6=severe)
- side effects (dryness, peeling, erythema, burning, perception of oiliness)
Patient ratings:
- how frequently moisturizer was used since last visit
- burning since last visit
- skin comfort (0=very comfortable, 5=very uncomfortable)
- compliance
Results: Baseline mean inflammatory lesion count for both groups was 22; mean noninflammatory lesion count was 36 (taz) and 38 (taz+moisturizer). Reduction in lesion count was similar between the tazarotene + moisturizer group and tazarotene-only group: 57% vs 46% for inflammatory lesions, and 50% vs 46% for non-inflammatory lesions. Reduction in overall severity score was also comparable between groups.
Compliance was "mostly" or "very compliant" in both groups; moisturizer use was significantly greater in the taz+moisturizer group (....that's good); taz-only group used moisturizer "a little" and "occasionally".
Side effects:
- no adverse events
- dryness was consistently lower in the taz+moisturizer group but were only significant at week 2 (p<0.01)
- peeling and erythema were consistently lower in the taz+moisturizer group (not significant)
- burning similar between groups
- perception of oiliness was similar between groups
Conflicts of Interest: Supported by Allergan
Notes: Sorry for choosing the poster option, it's basically already in summary format! It's awesome that buffering didn't significantly mess with efficacy, although I'd like to see the full study.
[7] Gentle cleansers and moisturizers are key to treating acne.
Title (Year). Authors: Del Rosso, James Q. “The role of skin care as an integral component in the management of acne vulgaris: part 1: the importance of cleanser and moisturizer ingredients, design, and product selection” Journal of clinical and aesthetic dermatology vol. 6,12 (2013): 19-27.
Title (Year). Authors: Del Rosso, James Q and Staci Brandt. “The Role of Skin Care as an Integral Component in the Management of Acne Vulgaris: Part 2: Tolerability and Performance of a Designated Skin Care Regimen Using a Foam Wash and Moisturizer SPF 30 in Patients with Acne Vulgaris Undergoing Active Treatment” Journal of clinical and aesthetic dermatology vol. 6,12 (2013): 28-36.
Summary: This wasn’t a study so much as a summary of existing literature and the author’s own clinical experience treating patients with acne. It can be summed up in the following way: fancy treatments are important, but skin health also matters and cleansers and moisturizers are super important too. Hilariously the author also described doing a web search on “Ask Jeeves” for ““What are the best treatments for acne?”. The author goes on to critique the page and the recommendations there, and basically advises doctors that this is where patients are getting their information from. “Dermatologists need to be keenly aware that the internet and many other sources of information that do not evaluate the patient with [acne] and other conditions are commonly consulted and trusted by the public.”
Conflicts of interest: Author has worked with a bunch of pharmaceutical companies (Allergen, Bayer, etc. etc. etc.) but none of them were involved in this write-up.
[8] Tretinoin + niacinamide is better for improving wrinkles, pigmentation, and texture than tretinoin alone.
Title (Year). Authors: Draelos, Zoe Diana. "Clinical situations conducive to proactive skin health and anti-aging improvement." Journal of Investigative Dermatology Symposium Proceedings. Vol. 13. No. 1. Elsevier, 2008.
Summary: “barrier-enhancing skin cleansers and moisturizers can both maintain and aid in the restoration of skin health”
Study 1: 41 adult female subjects (n=41) were treated with control versus 2% niacinamide for their forearm skin for 24 days, and TEWL was determined at day 1, day 12, day 19 and day 24. The 2% niacinamide treatment had statistically significantly less trans-epidermal water loss (they were less dry).
Study 2: 50 people used tretinoin plus a basic moisturizer, or tretinoin plus a niacinamide-enhanced moisturizer for 8 weeks. The researchers assessed them for photodamage at baseline and after the 8-week treatment. The moisturizer with niacinamide showed more improvement for every measure: fine lines/wrinkles, mottled pigmentation, blotchiness, and texture.
Conflicts of interest: Author was paid an honorarium by Proctor and Gamble for writing up this paper. The studies themselves were done independently and this was just a review of all the related work.
Notes: Holy cow I am surprised at what a difference niacinamide makes!! Definitely add some niacinamide to your routine if you don’t already have some.
[9] Using a moisturizer with ceramides makes tretinoin hurt less.
Title (Year). Authors: Schorr, Ethlynn S., Farzi Sidou, and Nabil Kerrouche. "Adjunctive use of a facial moisturizer SPF 30 containing ceramide precursor improves tolerability of topical tretinoin 0.05%: a randomized, investigator-blinded, split-face study." Journal of drugs in dermatology: JDD 11.9 (2012): 1104-1107.
Study: No idea how many participants, their age/gender/etc, or how long it was run for. Investigator/evaluator-blinded, split-face comparison in subjects with healthy skin. Participants applied tretinoin to their entire face, then moisturizer to half their face. Majority of participants (~84%-86%) experienced only mild irritation on the side that got moisturized.
[10] Retinoid-Induced Flaring in Patients with Acne Vulgaris: Does It Really Exist?
Title (Year). Authors: Del Rosso, James Q., and F. A. O. C. D. Tretinoin. "Retinoid-induced flaring in patients with acne vulgaris: does it really exist." J Clin Aesthet Dermatol 1.1 (2008): 41-43
[14] Acne lesion count decreases over 12 weeks.
Thiboutot, D., Pariser, D., Egan, N., Flores, J., Herndon, J., & Kanof, N. et al. (2006). Adapalene gel 0.3% for the treatment of acne vulgaris: A multicenter, randomized, double-blind, controlled, phase III trial. Journal Of The American Academy Of Dermatology, 54(2), 242-250. doi:10.1016/j.jaad.2004.10.879
[15] Short-contact therapy shows ~50% decrease in acne lesions over 12 weeks (tazarotene).
Bershad, S., Singer, G., Parente, J., Tan, M., Sherer, D., Persaud, A., & Lebwohl, M. (2002). Successful Treatment of Acne Vulgaris Using a New Method. Archives Of Dermatology, 138(4). doi:10.1001/archderm.138.4.481
[16] Expect to see lesion decrease after 8 weeks (0.05% tretinoin gel).
Chalker, D., Lesher, J., Smith, J., Klauda, H., Pochi, P., & Jacoby, W. et al. (1987). Efficacy of topical isotretinoin 0.05% gel in acne vulgaris: Results of a multicenter, double-blind investigation. Journal Of The American Academy Of Dermatology, 17(2), 251-254. doi:10.1016/s0190-9622(87)70200-x
[29] Oiliness decreases after 3 months for both 0.1% adapalene and 0.025% tretinoin
Ellis, Millikan, Smith, Chalker, Swinyer, & Katz et al. (1998). Comparison of adapalene 0 ·1% solution and tretinoin 0 ·025% gel in the topical treatment of acne vulgaris. British Journal Of Dermatology, 139, 41-47. doi:10.1046/j.1365-2133.1998.1390s2041.x
Hyperpigmentation
[17] Time frame for hyperpigmentation improvement is 9 months (0.1% tretinoin)
Bulengo-Ransby, S., Griffiths, C., Kimbrough-Green, C., Finkel, L., Hamilton, T., Ellis, C., & Voorhees, J. (1993). Topical Tretinoin (Retinoic Acid) Therapy for Hyperpigmented Lesions Caused by Inflammation of the Skin in Black Patients. New England Journal Of Medicine, 328(20), 1438-1443. doi:10.1056/nejm199305203282002
[18] 0.1% Tazarotene is approximately as effective as 0.05% tretinoin for hyperpigmentation and fine wrinkles after 6 months.
Kang, S., Leyden, J., Lowe, N., Ortonne, J., Phillips, T., & Weinstein, G. et al. (2001). Tazarotene Cream for the Treatment of Facial Photodamage. Archives Of Dermatology, 137(12). doi:10.1001/archderm.137.12.1597
[19] Both 0.05% and 0.1% tretinoin improve hyperpigmentation and fine lines over 6 months.
Olsen, E., Irving Katz, H., Levine, N., Shupack, J., Billys, M., & Prawer, S. et al. (1992). Tretinoin emollient cream: A new therapy for photodamaged skin. Journal Of The American Academy Of Dermatology, 26(2), 215-224. doi:10.1016/0190-9622(92)70030-j
[20] 0.5% tretinoin improved hyperpigmentation and fine lines over 6 months
Leyden, J., Grove, G., Grove, M., Thorne, E., & Lufrano, L. (1989). Treatment of photodamaged facial skin with topical tretinoin. Journal Of The American Academy Of Dermatology, 21(3), 638-644. doi:10.1016/s0190-9622(89)70231-0
[21] 0.1% tretinoin improves hyperpigmentation and fine lines over 9 months.
Also, topically-applied tretinoin can be detected in the blood, but doesn’t build up over time.
Maddin, S., Lauharanta, J., Agache, P., Burrows, L., Zultak, M., & Bulger, L. (2000). Isotretinoin improves the appearance of photodamaged skin: Results of a 36-week, multicenter, double-blind, placebo-controlled trial. Journal Of The American Academy Of Dermatology, 42(1), 56-63. doi:10.1016/s0190-9622(00)90009-4
Indented scars
[22] 0.3% adapalene improves indented scarring after 6 months.
Loss, M., Leung, S., Chien, A., Kerrouche, N., Fischer, A., & Kang, S. (2018). Adapalene 0.3% Gel Shows Efficacy for the Treatment of Atrophic Acne Scars. Dermatology And Therapy, 8(2), 245-257. doi:10.1007/s13555-018-0231-8
Aging
[6] The increased cell turnover triggered by tretinoin does not “use up” your cells early.
Discussion on Senescence (Long-term aging). This phenomenal write-up is by the wonderful /u/Feather-Light!
I've spent the last few hours reading the research on this topic, which was largely going through the studies of interest cited in this review of Hayflick limit research.
Terms to understand:
- *Cumulative Population Doublings (CPD)*: Hayflick claimed that a cell could divide 250 times, which is "more than enough cells for several lifetimes."
- *Replicative senescence (RS)*: The point at which a cell can no longer divide and does not respond to growth factor stimulation to divide.
- *In vitro*: Research done in a petri dish using cell cultures like fibroblasts.
- *In vivo*: Research done on living human subjects.
Basic concepts for the reader to understand:
- RS does not mean cell death. Cells do not die when they reach senescence. They merely stop dividing. They are still metabolically active.
- Do not conflate in vitro findings with in vivo findings. We are living human beings. We are not cell cultures in a petri dish. Do not equate what in vitro research finds to what *actually happens* in our bodies.
So you have to understand that Hayflick limit research is done in vitro. You also have to understand that RS was observed after a period of months. So do you see the disconnect here? Clearly we know our skin cells divide for far longer than a period of months that the in vitro Hayflick limit research has found. This is to say to not take in vitro research so literally. This is why our gold standard with anti aging studies are in vivo, so we know what actually happens in living humans, which is what we are, because again, we're not cell culture petri dishes.
A main takeaway here is that RS is often reached by many other means other than cellular division. Cytotoxic factors such as alcohol and radiation cause stress-induced premature senescence (SIPS). And of note here is that Hayflick's research used cell cultures with 20% oxygen to come up with that 250 figure. Actual physiological conditions in the human body are ~3% oxygen, which in vitro research using this parameter has reported a limit of 2^70. This demonstrates oxidative stress induces RS.
When we have RS due to cellular division, we see telomere shortening. But our gold standard of in vivo research on human subjects has shown that "studies in centenarians have raised doubts on whether telomere shortening occurs in vivo and whether senescence-associated genes in vitro are also differentially expressed in vivo." So basically, we see RS occurring not because of cellular division limits but because of stress inducers, such as oxidative stress. And oxidative stress is the whole concept of why UVA rays are bad: UVA rays generate reactive oxygen species (i.e. free radicals) and cause a negative chain reaction of cellular and DNA damage, thus the signs of premature aging which we call photoaging or sun damage.
The fact is that we're finding environmental stressors to be the cause of RS, not cellular division rates. So as a layperson who is merely a skincare research hobbyist and who constantly seeks out the knowledge to curate an optimized anti aging routine for fun, I'll absolutely keep on using retinoids and chemical exfoliants which we know increases the rate of skin cell turnover. And I'll certainly keep using an SPF 50+ PA++++ sunscreen to prevent the deleterious effects of UVA damage and its key role in oxidative stress.
I'll end this writeup quoting the review: "while there is little evidence to suggest that cells running out of divisions are a major factor in aging, it is possible that stress and various insults trigger cell senescence in vivo."
[23] 0.1% tretinoin decreases wrinkles after 3 months
Tretinoin increases epidermal thickness, and stimulates collagen.
Kong, R., Cui, Y., Fisher, G., Wang, X., Chen, Y., Schneider, L., & Majmudar, G. (2015). A comparative study of the effects of retinol and retinoic acid on histological, molecular, and clinical properties of human skin. Journal Of Cosmetic Dermatology, 15(1), 49-57. doi:10.1111/jocd.12193
[24] 0.4% retinol improves already-aged skin (doesn’t just prevent aging) after 6 months.
Kafi, R., Kwak, H., Schumacher, W., Cho, S., Hanft, V., & Hamilton, T. et al. (2007). Improvement of Naturally Aged Skin With Vitamin A (Retinol). Archives Of Dermatology, 143(5). doi:10.1001/archderm.143.5.606
[25] 0.05% tretinoin improves hyperpigmentation and fine wrinkles after 6 months.
Weinstein, G., Nigra, T., Pochi, P., Savin, R., Allan, A., Benik, K., Jeffes, E., Lufrano, L., & Thorne, E. (1991). Topical Tretinoin for Treatment of Photodamaged Skin. Archives Of Dermatology, 127(5), 659. doi:10.1001/archderm.1991.01680040067005
[26] 0.05% tretinoin improves wrinkles and hyperpigmentation after 3 months
Lever, L., Kumar, P., & Marks, R. (1990). Topical retinoic acid for treatment of solar damage. British Journal Of Dermatology, 122(1), 91-98. doi:10.1111/j.1365-2133.1990.tb08244.x
[27] Tretinoin improves photodamage after 4 months (unknown percentage)
Weiss, J. , Ellis, C. , Headington, J. , Tincoff, T. , Hamilton, T. , & Voorhees, J. (1988). Topical Tretinoin Improves Photoaged Skin. JAMA, 259(4), 527. doi:10.1001/jama.1988.03720040019020
[28] 0.05% tretinoin and 0.02% tretinoin both improves wrinkles and hyperpigmentation over 6 months
Nyirady, J., Bergfeld, W., Ellis, C., Levine, N., Savin, R., & Shavin, J. et al. (2001). Tretinoin cream 0.02% for the treatment of photodamaged facial skin: a review of 2 double-blind clinical studies. Cutis, 68(2), 135-142.
General
[11] Water increases skin permeability.
Barai, Namrata D. Effect of hydration on skin permeability. Diss. University of Cincinnati, 2002.
Summarizes current (as of 2002) knowledge around the role that hydration plays in skin permeability.
[14] Water increases absorption
Mojumdar, Enamul Haque, et al. "Skin hydration: interplay between molecular dynamics, structure and water uptake in the stratum corneum." Scientific reports 7.1 (2017): 1-13.
[12] Excessive hydration increases skin irritation
This is because excessive hydration causes changes in the skin structure of the stratum corneum.
Ogawa‐Fuse, Chie, et al. "Impact of water exposure on skin barrier permeability and ultrastructure." Contact Dermatitis 80.4 (2019): 228-233.
[13] Hydration helps molecules be absorbed by the skin
“Water is the most natural and biocompatible penetration enhancer known to improve the permeability of skin…we use cryo-scanning electron microscopy…” to study how changes in the stratum corneum (SC) affect the absorption of other molecules. “We clearly show that the SC is a dynamic structure, where extended hydration (>8 h) swells corneocytes, creates intercorneocyte ruptures, and causes microstructural changes in lipid self-assembly. The implications to biomacromolecule penetration are significant, since these disruptions allow penetration through the barrier of the SC.”
[30] Retinoids vary in strength
“Tazarotene is the strongest retinoid, while retinol is the weakest (retinyl palmitate is even weaker than retinol - more on that below*). The strength of a retinoid depends on the type of retinoid. Your skin is only able to use a retinoid when it's in retinoic acid form. Therefore, all types of retinoids are converted to this state by your skin before it can even be used. How does this have anything to do with a retinoid's strength? Allow me to explain.
When you apply a retinoid product that is retinoic acid (ex. Retin-A), your skin is able to use it immediately because it's already in the proper form. However, if you use a product with retinol, the retinol first has to be converted into retinaldehyde and then the retinaldehyde has to be converted to retinoic acid before your skin can use it. Therefore, retinol is weaker than retinaldehyde and retinaldehyde is weaker than retinoic acid. Retinol is the weakest of those three because it takes your skin two extra steps for it to be converted to retinoic acid before it can be utilized. For each conversion step, there is also some uncertainty as to how much of the retinoid was actually converted in the oxidation process (i.e. the retinol may not be 100% converted into retinoic acid). Therefore, the fewer the conversions it takes to get to retinoic acid, the stronger the retinoid.” skinacea.com
Tan, Grace, et al. "Hydration effects on skin microstructure as probed by high-resolution cryo-scanning electron microscopy and mechanistic implications to enhanced transcutaneous delivery of biomacromolecules." Journal of pharmaceutical sciences 99.2 (2010): 730-740.
Retinol vs Retinoic acid
Antiaging Action of Retinol: From Molecular to Clinical
- 0.1% retinol showed an increase in epidermal thickness, number of proliferating cells, cell turnover rate, and improves wrinkles, fine lines, and skin tone evenness. It's important to keep in mind that compared to the control group, retinol did significantly better only for fine lines at week 36 and for wrinkles at week 12.
Molecular basis of retinol anti‐ageing properties in naturally aged human skin in vivo.
- Small study comparing 0.4% retinol to control found increased epidermal thickness (2.1-fold), increased dermal vascularity, increased keratinocyte proliferation (12-fold), increased Type I collagen formation (3-fold), etc.
- looked at various concentrations of tretinoin and retinol (from 0.1% retinol to 1.6%)
- retinol did not cause significant erythema, whereas retinoic acid did. Despite the lack of irritation, retinol acts via similar pathways to retinoic acid and promote epidermal thickening.
Improvement of Naturally Aged Skin With Vitamin A (Retinol).
- 0.4% retinol (applied 3X weekly) significantly reduces fine wrinkles starting at ~8 weeks. The appearance of wrinkles further declines over time.
- Retinol increased epidermal thickness, gene expression, and procollagen types I and III. In the clinical study, 0.1% retinol significantly reduced facial wrinkles after 12 weeks
- 0.1% retinol moisturizer over 8 weeks can reduce the appearance of wrinkles and increase the apparent "firmness" of the skin. However, simple moisturizing without retinol can improve the appearance of your skin too, but not to the same extent as the retinol-containing moisturizer.
Studies that need summarizing
Message the moderators if you’d like to summarize one of these studies, or another one you’ve found!
- Rosso, James Del et al. “Tretinoin photostability: comparison of micronized tretinoin gel 0.05% and tretinoin gel 0.025% following exposure to fluorescent and solar light” Journal of clinical and aesthetic dermatology vol. 6,2 (2013): 25-8.
- Elbaum, David J. "Comparison of the stability of topical isotretinoin and topical tretinoin and their efficacy in acne." Journal of the American Academy of Dermatology 19.3 (1988): 486-491.
-
- Rocha, M. A., and E. Bagatin. "Skin barrier and microbiome in acne." Archives of dermatological research 310.3 (2018): 181-185.
- Bartlett, Kyle B., Scott A. Davis, and Steven R. Feldman. "Topical antimicrobial acne treatment tolerability: A meaningful factor in treatment adherence?" Journal of the American Academy of Dermatology 71.3 (2014): 581-582.
- Griffiths, Christopher EM, et al. "Two concentrations of topical tretinoin (retinoic acid) cause similar improvement of photoaging but different degrees of irritation: a double-blind, vehicle-controlled comparison of 0.1% and 0.025% tretinoin creams." Archives of dermatology 131.9 (1995): 1037-1044.
- Del Rosso, James Q et al. “Absence of Degradation of Tretinoin When Benzoyl Peroxide is Combined with an Optimized Formulation of Tretinoin Gel (0.05%)” Journal of clinical and aesthetic dermatology vol. 3,10 (2010): 26-8.
- Tretinoin Photostability. Comparison of Micronized Tretinoin Gel 0.05% and Tretinoin Gel 0.025% Following Exposure to Fluorescent and Solar Light https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3579485/
- - BP does not degrade tret [src](https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2958193/).
- A comparison between 0.025% and 0.1% shows similar improvement, but much less irritation for the lower percentage. [src](https://www.ncbi.nlm.nih.gov/m/pubmed/7544967/).
- [src](https://mdedge-files-live.s3.us-east-2.amazonaws.com/files/s3fs-public/Document/September-2017/078040275.pdf).
- Keep your skin moisturized and healthy to prevent breakouts and heal faster when you do break out. [src](https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3997205/)
- One study found a degradation of 11% after an 8-hr exposure to flourescent light [src](https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3579485/).
Research Summary Template
**Title (Year). Authors.**
**Variables:**
**Participants:**
**Methods:**
**Results:**
**Conflicts of Interest:**
**Notes:**
Make sure there are two spaces at the end of each line!
- Variable(s) of interest: what's the study looking at, exactly?
- Brief procedural run down: how was the study conducted?
- Participant type;
- Number of participants;
- Methods: how the variables were investigated
- Summary of the results - what did the study find?
- Conflicts of interest - generally found at the end of the paper in a disclosure statement
- Notes - your own thoughts about the study, including any potential methodological strengths/weaknesses
Excerpts from Leslie Baumann's Cosmetic Dermatology retinoids/tretinoin.
Generously shared by the kind and generous /u/S3mirmis
On indications:
Not surprisingly, she recommend tret for acne (p.122 and following) and to heal photoaging (p. 257 among others). On the preventation of aging you can read the following:
"[E]vidence suggests that it [tretinoin] also plays a role in the prevention of aging. This can be linked to inhibitory effects of retinoids on damaging metalloproteinases. UVB exposure dramatically upregulates the production of several collagen degrading enzymes known as matrix metalloproteinases (MMPs) (see Chapter 6). Activation of MMP genes results in production of collagenase, gelatinase, and stromelysin, which have been shown to fully degrade skin collagen17(Box 30-1). Fisher et al. demonstrated that application of tretinoin inhibits the induction of all three of these harmful MMPs.1 In addition to increasing levels of destructive enzymes such as collagenase, UV exposure has also been shown to decrease collagen production. Fisher et al. demonstrated that expression of collagen types I and III is substantially reduced within 24 hours after a single UV exposure. Pretreatment of the skin with all-trans-retinoic acid (tretinoin) was shown to inhibit this loss of procollagen synthesis. Therefore, pretreatment of the skin with topical retinoids, when used consistently, is likely to be beneficial in prevent-ing as well as treating photodamage." (p. 257)
On introducing tret and other misc:
- Patients with sensitive skin will be instructed by Dr. Baumann to use tret every third night for two weeks. If no redness occurs, up it to every other night for two weeks. If again no redness, increase usage to every night. (p.259)
- Patients with sensitive skin may also mix their tret 1:1 with a pea-sized amount of moisturizer (p. 259)
- Tret may only be used two times/week on the neck due to it being more sensitive (p. 259)
- If one uses BHA or AHA those should be applied with a wait time of 30min before the retinoid (p.259)
- Stop retinoid usage one week before waxing (p. 259)
- No Microdermabrasion, at home chemical peels or facial scrubs unless discussed with your provider first (p. 259)
- She of course mentions the importance of sunscreen at various occasions (duh)
- It takes 8 weeks to show first results in acne according to her (p. 122)
On frequency of usage
In the 1990s a study found that the benefits gained by using 0,05% tret daily for four years could be kept by using it 3 times a week for the next two years. using it only once a week was not enough to maintain the good results. The same study showed that the benefits would reverse themselves if one stops using tret altogether. Dr. Baumann follows that tret should be used at least three times a week. (p. 258, 259).
On side effects:
- Tret increases TEWL and causes dry skin (p. 259)
- It decreases the production of ceramides at least short-term (p. 259)
- The flaking that occurs in tret patients is caused by a different mechanism compared to what causes it in patient with very dry skin (p. 259)
- Using a barrier repair moisturizer is recommend to increase tolerability (p. 260)
Meta
Moderating philosophy
- Rules exist to help set community expectations.
- There’s no set of rules that will perfectly apply to all situations.
- We’re human and may make mistakes. If you ask us why we made a particular decision, we will always explain it.
- We try to stay “hands-off” as much as possible.
- We do not search the sub for rule-breakers - we’re not interested in enforcing rules for the sake of enforcing rules. If you - as a community member - want the rules enforced, help us enforce them by reporting posts!
- Please report posts that break the rules - it is anonymous and very helpful.