Legitimacy of the Religious Exemption from Vaccination on Pro-Life Grounds
Ongoing Use of Aborted Babies in Vaccine R & D:
We do not know exactly how many aborted babies have been used in the research and development of vaccines. It is commonly asserted that there were only two aborted babies, aborted decades in the past (the 60’s), and no more have been or will be utilized. However, the following sources testify that there were far more than two aborted babies involved, and the creation of cell lines derived from aborted babies for use in vaccine development has been/continues to be ongoing. Therefore, the number of aborted babies used in vaccine R & D is certainly not static, but continues to rise.
The following quotes are from “A Brief History of Human Diploid Cell Strains” by Dr. Rene Leiva originally published in the National Catholics Bioethics Quarterly in Autumn 2006 by the National Catholic Bioethics Center. All information in this source is impeccably cited by its author, and I will include these citations:
“Even though there are many cell strains in use in research, the most well known are WI-38 and MRC-5. These two cell strains come from two deliberately aborted fetuses. But as the evidence shows, there were more abortions involved to achieve the technical expertise needed for development of these cell strains. In addition, other cell strains have been developed for vaccine manufacturing and other pur-poses. Because of its relevance to this discussion, I will also review the history of the virus strain RA 27/3, as it is the source of the only rubella vaccine available in NorthAmerica and in fact, most of the world.” p. 2
“The Wistar Institute is a scientific institute located on the campus of the University of Pennsylvania in Philadelphia, specializing in the fields of immunology and cell biology. Working for the Institute in 1961, Dr. Leonard Hayflick first published a paper describing twenty-five HDCS: WI-1 through WI-25 (Wistar Institute fetal samples nos. 1–25). These cell strains were derived from the lung, skin, muscle, kidney, heart, thyroid, thymus and liver of nineteen separate, electively-aborted fetuses.” p. 2
(via L. Hayflick and P. S. Moorhead, “The Serial Cultivation of Human Diploid CellStrains,” Experimental Cell Research 25.3 (December 1961): 618.)
“Abortion was illegal in the United States at that time, so fetal tissue was provided by Dr. Sven Gard of the Karolinska Institute Medical School in Stockholm, Sweden. Dr. Erling Norrby, who later served as chairman of the department of virology and dean of the medical faculty at the Karolinska Institute, was a graduate student there during this period. He dissected many of the aborted fetuses:
‘My predecessor as professor of virology at the Karolinska Institute in Stockholm, Sven Gard, spent a sabbatical year at the Wistar Institute in 1959, two years after the institution had been taken over by the dynamic Koprowski. One of my duties as a young student in the laboratory in Stockholm was to dissect human fetuses from legal abortions and send organs to the Wistar Institute. Such material was the source of many important studies of cell lines at the Institute, such as Leonard Hayflick’s study of WI-38 cells.’” p. 2-3
(via E. Norrby, “Listen to the Music: The Life of Hilary Koprowski (review),” Perspectives in Biology and Medicine 44.2 (Spring 2001): 304; Fletcher, Hessel, and Plotkin,“Human Diploid Cell Strains,” 97–98; and Norrby, “Listen to the Music,” 304.)
“Hayflick published his reports of the development of WI-38. WI-38 was obtained from a three-month-old female fetus...This report also mentions two additional cell strains: WI-26 from a male fetus (lung) and WI-44 from a female fetus (lung). Both fetuses were about three-months’ gestation as well.” p. 3
(via Hayflick et al., “Preparation of Poliovirus Vaccines,” 240, 244, 254)
“Dr. J. P. Jacobs published the development of the cell strain MRC-5 (Medical Research Council strain no. 5) in 1970. He replicated Hayflick’s work with the purpose of creating cells strains for the production of vaccines:
‘The stability and integrity of the human foetal cell strain WI-38 ... explain the value of such material for the isolation of viruses and in the development of vaccines. We have developed another strain of cells, also derived from fetal lung tissue, taken from a fourteen-week male fetus removed for psychiatric reasons from a twenty-seven-year-old woman with a genetically normal family history and no sign of neoplastic disease both at abortion and for at least three years afterwards.’
(via J. P. Jacobs, C. M. Jones, and J. P. Baille, “Characteristics of a Human DiploidCell Designated MRC-5,” Nature 227.5254 (July 11, 1970): 168.)
“There is the possibility that there may have been previous abortions performed to create MRC-5. In fact, Jacobs reported creating a second cell strain, MRC-9, by the use of a different aborted fetus:
‘the cells were derived from the lungs of a female fetus in 1974, whose gestational age was about fifteen weeks. The fetus was of normal development andwas delivered of a fourteen-year-old mother whose pregnancy was terminatedby therapeutic abortion because she was unmarried. The medical history of the mother and her family indicated nothing abnormal according to information given by the gynecologist who performed the operation. The lungs were dissected from the fetus immediately following the abortion…’” p. 4
(via J. P. Jacobs, A. J. Garrett, and R. Merton, “Characteristics of a Serially PropagatedHuman Diploid Cell Designated MRC-9,” Journal of Biological Standardization 7.2 (April1979): 114.)
“Newer HDCSs continued to be made as back-ups for the current cell strains. Among the most common ones are IMR-90, cell strain 293, and PER C6.15 In short, IMR-90 was established from a sixteen-week-old human fetus on July 7, 1975, from a therapeutic abortion performed on a thirty-eight-year-old white mother of six. Cell strain 293 was made from human embryonic kidney cells from an aborted fetus in 1972, and cell strain PER C6 from human embryonic retina cells from an abortion in 1985. The main researcher was Dr. A. J. van der Eb at Leiden University in Holland...Van der Eb stated that ‘PER C6 was made just for the pharmaceutical manufacturing of adenovirus vectors.’...Cell strain 293 was made for ‘basic research.’ At least fifty companies have licensed PER C6, including Merck, the sole manufacturer of the only rubella vaccine available in North America.” p. 5
(via W. W. Nichols et al., “Characterization of a New Human Diploid Cell Strain, IMR-90,” Science 196.4285 (April 1, 1977): 60; FDA Vaccines and Related Biological ProductsAdvisory Committee, transcript of meeting May 16, 2001, “Session on Designer Cell Substrate,” http://www.fda.gov/ohrms/dockets/ac/01/transcripts /3750t1 01.pdf.; Nichols et al., “Characterization of a New Human Diploid Cell Strain,” 60.; Alex J. van der Eb, in “Session on Designer Cell Substrates,” FDA meeting transcript, May 16, 2001.; and L. Xie et al., “Large-Scale Propagation of a Replication-Defective Adenovirus Vector in Stirred-Tank Bioreactor PER.C6 Cell Culture under Sparging Conditions,” Biotechnology and Bioengineering 83.1 (July 5, 2003): 45.)
“Currently, the virus strain (RA 27/3) found in the rubella vaccine most commonly used around the world was developed by Dr. Stanley Plotkin and colleagues at the Wistar Institute. The RA 27/3 (rubella abortus, twenty-seventh fetus, third tissue extract) virus strain was obtained from a female human fetus in a series of twenty-seven abortions in the United States: ‘Explant cultures were made of the dissected organs of a particular fetus aborted because of rubella, the twenty-seventh in our series of fetuses aborted during the 1964 epidemic.’” p. 5
(via S. A. Plotkin, D. Cornfeld, and T.H. Ingalls, “Studies of Immunization with Living Rubella Virus: Trials in Children with a Strain Cultured from an Aborted Fetus,” AmericanJournal of Diseases of Children 110.4 (October 1965): 381–382.; and S. A. Plotkin et al., “Attentuation of RA 27-3 Rubella Virus in WI-38 Human Dip-loid Cells,”American Journal of Disabilities of Children 118.2 (August 1969): 178.)
“Additionally, six months after publishing this research, Plotkin and colleagues published an article documenting forty, not twenty-seven, abortions:
‘Out of the forty rubella fetuses cultured, cell strains were derived from thirty-four; in most cases they originated from pieces of skin and muscle obtained at curettage ... rubella virus was isolated from the supernatant culture medium of cell strains derived from eighteen fetuses; sixteen fetuses yielded cell strains which were rubella negative.’” p. 6
(via T. H. Chang et al., “Chromosome Studies of Human Cells Infected in Utero and InVitro with Rubella Virus,” Proceedings of the Society for Experimental Biology and Medicine 122.1 (May 1966): 237–238.)
“Later, Drs. J. Hoskins and Plotkin tested the action of the RA 27/3 virus on different systems of human embryonic cell cultures. Additional cell strains weremade from more fetuses originating in both elective abortions (twenty-one) andmiscarriages (seven)..” p. 6
(via J. M. Hoskins and S. A. Plotkin, “Behaviour of Rubella Virus in Human Diploid CellStrains. I.Growth of Virus,” Archiv fur die Gesamte Virusforschung 21.3 (1967): 285; J.M. Hoskins and S. A. Plotkin, “Behaviour of Rubella Virus in Human Diploid Cell Strains. II.Studies of Infected Cells,” Archiv fur die Gesamte Virusforschung 21.3 (1967): 297.)
“There is clear evidence that research around the development of the RA 27/3 rubella vaccine included the performance and coordination of at least eighty abortions, including the two individual abortions for the creation of WI-38 and RA 27/3. Development of MRC-5 used one abortion, but there is a strong indication that more abortions occurred...Pharmaceutical companies are actively involved in this research and new vaccines are being made with unethical cell strains.” p. 8-9
(via M. N. Oxman et al. for the Shingles Prevention Study, “A Vaccine to Prevent Her-pes Zoster and Postherpetic Neuralgia in Older Adults,” New England Journal of Medi-cine 352.22 (June 2, 2005): 2271–2284.)
Additional sources:
- Video footage of Stanley Plotkin’s deposition, under oath, in which he confirms that in the one study that is being referred to alone, 76 aborted babies were involved. The plaintiff’s lawyer asks Dr. Plotkin:
“Are you aware that one of the objections to vaccination by the plaintiff in this case is the inclusion of aborted fetal tissue in the development of vaccines and the fact that it’s actually part of the ingredients of vaccines?”
To which Plotkin responds:
“I’m aware of those objections. The Catholic Church has actually issued a document on that which says that individuals who need vaccines should receive the vaccines regardless of the fact and, I think it implies that I am the individual who will go to hell because of the use of aborted tissues, which I am glad to do.”
https://www.youtube.com/watch?v=PN7FQCkiBp8&feature=youtu.be
- The complete transcript of Stanley Plotkin’s videotaped deposition in the trial above, State of Michigan in the Circuit Court for the County of Oakland Family Division, Lori Matheson vs Michael Schmitt, January 11, 2018, can be accessed here:
https://www.docdroid.net/8zJh4QQ/1-11-18-matheson-plotkin.pdf
- According to the World Health Organization, “Recommendations for the evaluation of animal cell cultures as substrates for the manufacture of biological medicinal products and for the characterization of cell banks,” by definition, human diploid cell strains (or DCLs) are finite, and will not last forever, in contradistinction to continuous cell lines (CCLs) which are “immortal”:
“Diploid cell line (DCL): A cell line having a finite in vitro lifespan in which the chromosomes are paired (euploid) and are structurally identical to those of the species from which they were derived.” p. 11
“Continuous cell line (CCL): A cell line having an apparently unlimited capacity for population doublings. Often referred to as ‘immortal’ and previously referred to as ‘established’”. p. 10
“Comparison of WI-38, MRC-5, and IMR-90 cell strains for isolation of viruses from clinical specimens,” published in the Journal of Clinical Microbiology in 1978 makes clear that the cell lines used in vaccine production are not considered immortal, nor infinite in supply:
“With the diminishing supply of the human fetal lung WI-38 cell strain, a replacement for viral isolation is needed. Two candidates are the human fetal lung strains MRC-5 and IMR-90.”
“MRC-5 and WI-38 cells remained healthy until generation 36, whereas IMR-90 cells went into crisis by generation 20. The longer life span of the MRC-5 cells makes them more suitable than IMR-90 cells to replace the WI-38 strain for routine use in viral diagnosis.”
“The human cell line PER.C6 provides a new manufacturing system for the production of influenza vaccines” published in March, 2001 states:
“Influenza viruses for vaccine production are currently grown on embryonated eggs. This manufacturing system conveys many major drawbacks such as inflexibility, cumbersome down stream processing, inability of some strains to replicate on eggs to high enough yields, and selection of receptor-binding variants with reduced antigenicity. These limitations emphasize the need for a cell line-based production system that could replace eggs in the production of influenza virus vaccines in a pandemic proof fashion. Here we present the efficient propagation of influenza A and B viruses on the fully characterized and standardized human cell line PER.C6.”
- WALVAX-2 is the newest human diploid cell line derived from an aborted baby and slated for use in vaccine R & D. It is discussed in “Characteristics and viral propagation properties of a new human diploid cell line, walvax-2, and its suitability as a candidate cell substrate for vaccine production” published in the journal Human Vaccines & Immunotherapeutics, in May 2015. Excerpts follow:
“Human diploid cell strains (HDCSs), possessing identical chromosome sets known to be free of all known adventitious agents, are of great use in developing human vaccines. However it is extremely difficult to obtain qualified HDCSs that can satisfy the requirements for the mass production of vaccines. We have developed a new HDCS, Walvax-2, which we derived from the lung tissue of a 3-month-old fetus.”
“Specifically, Walvax-2 cells replicated more rapidly than MRC-5 cells, with Walvax-2 cells attaining the same degree of confluence in 48 hours as was reached by MRC-5 cells in 72 hours. Moreover, Walvax-2 cells attained 58 passages of cell doublings whereas MRC-5 reached 48 passages during this period. We also assessed the susceptibility of these cells to rabies, hepatitis A, and Varicella viruses. Analysis of virus titers showed the Walvax-2 cells to be equal or superior to MRC-5 cells for cultivating these viruses. Furthermore, in order to characterize the Walvax-2 cell banks, a series of tests including cell identification, chromosomal characterization, tumorigenicity, as well as tests for the presence of microbial agents, exogenous viruses, and retroviruses, were conducted according to standard international protocols. In conclusion, results from this study show that Walvax-2 cell banks are a promising cell substrate and could potentially be used for the manufacturing of HDCVs.”
“Due to the diminishing supply of WI-38, the MRC-5 line has become the most widely used cell strain in the production of HDCS-derived human vaccines. China consequently confronts 2 key challenges for the production of viral vaccines from MRC-5 cells (which are mainly obtained from abroad): concerns about influences of limited passages, and the policies of the countries from which the cells are imported. More specifically, the numbers of passages of the imported MRC-5 cells are generally higher, generally later than the 20th passage, resulting in restricted mass production due to decreased growth vitality. Additionally, according to the standard for the Pharmacopoeia of the People's Republic of China (2010), Volume III, the use of the HDCSs is limited to generations within 2-thirds of the primary cell lifespan for the manufacture of vaccines… Furthermore, the productive cell generations for the OKA-HDC on the Chinese market from 3 manufactures are MRC-5 cells in the 32nd and 33rd passages, which have therefore already reached the limit required as described above in Chinese Pharmacopeia (the 33rd passage is the last cell doubling that could be used in the production for the MRC-5). Relying on imported HDCSs, may lead to unstable supply as well as unpredictable costs. Therefore the intention of this study is to develop a completely new HDCS of Chinese origin that could be used in manufacturing viral vaccines.”
“We obtained 9 fetuses through rigorous screening based on carefully specified inclusion criteria (see Methods section). The Walvax-2 strain of cells met all of these criteria and proved to be the best cell line following careful evaluation. Therefore it was used for establishing a human diploid cell strain. Walvax-2 was derived from a fetal lung tissue, similar to WI-38 and MRC-5, and was obtained from a 3-month old female fetus aborted because of the presence of a uterine scar from a previous caesarean birth by a 27-year old healthy woman.”
“In conclusion, we have successfully established and characterized a new human diploid cell line designated Walvax-2, and evaluated its susceptibility to 3 kinds of viral vaccine strains. The Walvax-2 cells are equally susceptible, and in some cases superior to, the MRC-5 line for the cultivation of viruses. Results from this study suggest that the Walvax-2 cell banks are a promising cell substrate and could potentially be used for the manufacturing of HDCVs.”
- The 2015 PBS article, “Scientists say fetal tissue remains essential for vaccines and developing treatments,” makes clear that “anti-abortionists” are considered an obstruction to the pro-vaccine cause:
“The furor on Capitol Hill over Planned Parenthood has stoked a debate about the use of tissue from aborted fetuses in medical research, but U.S. scientists have been using such cells for decades to develop vaccines and seek treatments for a host of ailments, from vision loss and neurological disorders to cancer and AIDS.”
“From 2011 through 2014 alone, 97 research institutions — mostly universities and hospitals — received a total of $280 million in federal grants for fetal tissue research from the National Institutes of Health. A few institutions have consistently gotten large shares of that money, including Yale, the University of California and Massachusetts General Hospital, which is affiliated with Harvard.”
“Vaccines have been one of the chief public benefits of fetal tissue research.”
“Fetal tissue was ‘absolutely critical’ to the development of a potential Ebola vaccine that has shown promise, said Dr. Carrie Wolinetz, an associate director at NIH, which last year handed out $76 million for work involving fetal tissue, or 0.2 percent of the agency’s research budget.”
Multiple authoritative sources make clear that cell lines derived from aborted babies are considered to be superior, for many reasons, to ethically sourced cell lines. It is necessary to confirm this fact in order to establish that vaccine researchers and manufacturers will not opt, of their own accord, to supply vaccines sourced from ethical lines. This fact establishes the legitimacy of the religious exemption from vaccination on pro-life grounds, both as means of applying an economic/financial force driving manufacturers to license ethically sourced alternatives, and as a means of avoiding the use of morally reprehensible products in the interim.
- “Characteristics and viral propagation properties of a new human diploid cell line, walvax-2, and its suitability as a candidate cell substrate for vaccine production” :
“Antibodies produced for most kinds of viral diseases when the immune system is stimulated by intact viral particles. Owing to this property, the vast majority of viral vaccines still adopt the traditional cell substrate culture method. Three cell substrates, human diploid cells, continuous cell lines and primary cell lines, are always used for developing vaccines. However, continuous and primary cell lines used for vaccine production suffer from the limitation of being potentially strongly tumorigenic. Four Additionally the primary cell lines, which are obtained from animals, introduce potentially risky exogenous agents. In contrast, human diploid cell strains (HDCSs), acquired from embryos or other tissue cells of human origin, possess identical chromosome sets that are free of all known adventitious agents. These unique properties explain the value of such materials and the current interest in their use in the development of human viral vaccines. Human diploid cell vaccines (HDCVs) have been licensed all over the world. Many studies have demonstrated superior immunogenicity and safety of HDCVs relative to those using any other tissue culture, such as hamster kidney cells or vero cell vaccines. The WHO recommends HDCS as the safest cell culture substrate for the production of viral vaccines and consequently they have become the preferred cell substrate for vaccine production worldwide.”
“The essential features of DCLs of human (e.g., WI-38, MRC-5)...origin are: (a) they are cells passaged from primary cultures that have become established as cell lines with apparently stable characteristics over numerous PDLs [population doubling level]; (b) they have a finite capacity for serial propagation, which ends in senescence, a state in which the culture ceases to replicate, the cells remain alive and metabolically active, but may show morphological and biochemical changes some of which begin to appear before replication ceases; (c) they are non-tumourigenic; and (d) they display diploid cytogenetic characteristics with a low frequency of chromosomal abnormalities of number and structure until they enter senescence. Substantial experience since the 1960s has been accumulated on the cytogenetics of WI-38 and MRC-5, and ranges of expected frequencies of chromosomal abnormalities have been published.” p. 14
“Advantages: (a) they can be well characterized and standardized; (b) production can be based on a cryopreserved cell-bank system that allows for consistency and reproducibility of the reconstituted cell populations. A cell-bank system usually consists of cell-banks of defined population doubling or passage levels that generally include a MCB [master cell bank] and a working cell-bank (WCB); and (d) unlike the CCLs and SCLs [stem cell lines] discussed below, DCLs are not tumourigenic and therefore do not raise the potential safety issues associated with CCLs and SCLs.” p. 15
- “A Brief History of Human Diploid Cell Strains” by Dr. Rene Leiva originally published in the National Catholics Bioethics Quarterly in Autumn 2006 by the National Catholic Bioethics Center:
“Human diploid cell strains (HDCSs) are batches of cells that are currently used for different purposes, including culturing viruses for the manufacturing of vaccines. HDCS-derived human vaccines have been licensed worldwide for polio IVP and OVP, rabies, rubella, measles, varicella-zoster, mumps, and hepatitis A. Current vaccines contain extremely small traces of the original fetal DNA, while the cell strains contain the complete fetal chromosomal set. The choice of HDCS was made among several based on their susceptibility to many human viruses, their good characterization, the enormous number of cells obtained from one original culture, their long storage potential, the low cost of cell procurement, an excellent record of safety, and the very low risk of latent virus on the cells themselves.” p. 1-2
(via M. A. Fletcher, L. Hessel, and S. A. Plotkin, “Human Diploid Cell Strains (HDCS)Viral Vaccines,” Developments in Biological Standardization 93 (1998): 97–107;L. Hayflick, “History of Cell Substrates Used for Human Biologicals,” Developments inBiological Standardization 70 (1989): 11–26.)
- “The History of Vaccines: An Educational Resource by the College of Physicians of Philadelphia” explains:
“Animals have been used in the industrialized production of human vaccines since vaccine farms were established to harvest cowpox virus from calves in the late 1800s...Although many vaccines and anti-toxin products were successfully developed this way, using animals in vaccine development – particularly live animals – is not ideal. Research animals are costly and require extensive monitoring, both to maintain their health and to ensure the continued viability of the research. They may be carrying other bacteria or viruses that could contaminate the eventual vaccine, as with polio vaccines from the mid 20th century that were made with monkey cells and eventually found to contain a monkey virus called SV40, or Simian Virus 40...Moreover, some pathogens, such as the chickenpox virus, simply do not grow well in animal cells.”
“Even when vaccine development is done using animal products and not live animals – such as growing influenza vaccine viruses in chicken eggs – development can be hindered or even halted if the availability of the animal products drops. If an illness were to strike the egg-producing chickens, for example, they might produce too few eggs to be used in the development of seasonal flu vaccine, leading to a serious vaccine shortage. (It’s a common misconception that influenza vaccines could be produced more quickly if grown in cell cultures compared to using embryonated chicken eggs. In fact, growing the vaccine viruses in cell cultures would take about the same amount of time. However, cell cultures do not have the same potential availability issues as chicken eggs.)”
“For these and other reasons, using cell culture techniques to produce vaccine viruses in human cell strains is a significant advance in vaccine development.”
“Although it has now been used in the United States for more than 30 years, Plotkin’s rubella vaccine was initially ignored by the U.S. Food and Drug Administration in favor of rubella vaccines developed using duck embryo cells and dog kidney cells. In the late 1960s, there was concern in the country that a vaccine developed using human cells could be contaminated with other pathogens, though this concern was not supported by documented evidence. This is interesting in light of the discovery earlier in the decade that polio vaccines developed using primary monkey kidney cells were contaminated with simian viruses: this was one of the reasons researchers began using the normal human cell strain WI-38 in the first place. According to Hayflick, however, the main reason for using WI-38 was the fact that it could be stored in liquid nitrogen, reconstituted, and tested thoroughly before use for contaminating viruses. (None has ever been found in WI-38.) Primary monkey kidney cells could not be frozen and then reconstituted for testing as this would violate the concept of primary cells--originally the only class of cells allowed by the FDA to produce human virus vaccines.”
“Human fetal cells were valuable in fetal research because they support the growth of many human viruses and are sterile; they were first used around the time that researchers found that primary monkey kidney cells were contaminated with SV40 virus.”
“Life in vaccine science – a conversation with Stanley Plotkin at the 4th Conference on Vaccines in Dubrovnik, Croatia, September 2017,” published in Euro Surveill, April 2018. Excerpts:
“SM [interviewer]: The use of human diploid cells as a cell population of choice, and development of WI-38 and MRC-5 was controversial?”
“SP [Stanley Plotkin]: It was controversial for two reasons. One was that there was this fear that in human cells, there might be some hidden virus that would cause problems. You have to remember that at about the same time, SV40 was discovered in monkey cells. Since that was surprise, people were afraid that the same thing might be true for human cells. A second issue was a religious issue. Fetal cells had been isolated from an aborted fetus in Sweden, and since it was an aborted fetus, there was, let’s say, some issues with the Catholic Church. Going back to the first issue, a lot of work was done to show that the cells do not have any contaminating viruses, and indeed were, for that reason, safer than many other cells being used to make vaccines. The second issue, as far as the religious issue was concerned, the church decided that the only one who had sinned was me; that people who used the vaccine were free of sin because they were just using something that somebody else had developed. So, those were the controversies.”
- The Embryo Project Encyclopedia “Stanley Alan Plotkin (1932-),” published in April 2017 and supported by the National Science Foundation, Arizona State University, Center for Biology and Society, the Max Planck Institute for the History of Science in Berlin, and the MBL WHOI Library:
“Diploid human cells, like the WI-38 cells that Plotkin used, have the same number of chromosome pairs as typical human body cells. Plotkin argued that diploid human cells were a better medium for growing weakened virus strains for vaccines because they better represented the human cells to be vaccinated.”
“Plotkin’s primary opposition at the conference was Albert Sabin, who had successfully created an oral polio vaccine…that was widely used in the Soviet Union…He [Plotkin] further asserted that Sabin’s objections came from religious, not factual, reasons due to the origin of the WI-38 cells in aborted fetal tissues.”
- The Congressional Research Service’s “Fetal Tissue Research FAQs” clarifies that elective abortions are specifically preferred to miscarriages, etc:
“Fetal tissue used in research is obtained from elective abortions. Under certain rare circumstances, fetal tissue may also be obtained from a miscarriage, also called a spontaneous abortion, or following the removal of an ectopic pregnancy, which occurs when an embryo has implanted outside the uterus. Because the timing or recognition of a spontaneous abortion or ectopic pregnancy is unpredictable, and both conditions may result in a serious health emergency for the woman, the fetal tissue collected under these circumstances is often not suitable for research purposes.” p. 5
Ethical Dilemmas Multiply:
An additional ethical dilemma arises for the pro-life advocate with regard to the recognized protocol for obtaining permission from a mother who is considering legally aborting her baby, to donate her baby for research purposes, which includes those babies that will be designated for vaccine R & D. It is generally agreed that within the context of legal abortion, ethical donations can only be ensured by performing the abortion prior to receiving consent to donate. However, due to the extremely short window of time for appropriately handling the baby in order to remain viable for research, the consent to donate must unavoidably precede the decision to abort. In other words, there is no possible way to know whether this has factored into a woman’s decision or not.
- Excerpts from the NIH Grants Policy Statement:
“Current federal laws and regulations require informed consent for research involving the transplantation of human fetal tissue and for research with human fetal material associated with information that can identify a living individual. Most states require informed consent for the use of fetal tissue in research. Accordingly, NIH expects informed consent to have been obtained from the donor for any NIH-funded research using human fetal tissue. When obtaining primary human fetal tissue for research purposes, NIH expects grantees and contractors to maintain appropriate documentation, such as an attestation from the health care provider or a third party supplier, that informed consent was obtained at the time of tissue collection.”
“Sections 498A and 498B contain additional requirements for research on the transplantation of human fetal tissue for therapeutic purposes conducted or supported by NIH. Under section 498A, the official who signs the application is certifying that the research on transplantation of human fetal tissue will adhere to the following provisions:
- The woman who donates the fetal tissue must sign a statement declaring that the donation is being made:
- for therapeutic transplantation research,
- without any restriction regarding the identity of individuals who may receive the transplantation, and
- without the donor knowing the identity of the recipient.
- The attending physician must sign a statement that he/she has:
- obtained the tissue in accordance with the donor's signed statement and
- fully disclosed to the donor his or her intent, if any, to use the tissue in research and any known medical risks to the donor or risks to her privacy associated with the donation that are in addition to risks associated with the woman's medical care.
- In the case of tissue obtained pursuant to an induced abortion, the physician's statement also must state that he/she:
- obtained the woman's consent for the abortion before requesting or obtaining consent for the tissue to be used;
- did not alter the timing, method, or procedures used to terminate the pregnancy solely for the purpose of obtaining the tissue for research; and
- performed the abortion in accordance with applicable State and local laws.
- The PD/PI must sign a statement certifying that he/she is aware that the tissue is human fetal tissue obtained in a spontaneous or induced abortion, or pursuant to a stillbirth and that the tissue was donated for research purposes. The PD/PI also must certify that this information has been shared with others who have responsibilities regarding the research and, before eliciting informed consent from the transplantation recipient, will obtain written acknowledgment that the patient is aware of the aforementioned information.
- The PD/PI must certify in writing that he/she has had no part in any decisions as to the timing, method, or procedures used to terminate the pregnancy.”
- The protocol above are echoed in the Congressional Research Service Fetal Tissue Research FAQs (p. 6-8), the American Medical Association “Research Using Fetal Tissue”, and “Biomedical Politics” published by the Institute of Medicine Committee to Study Decision Making, National Academies Press, 1991.
- Included as a footnote in Dr. Alvin Wong’s “Ethics of HEK 293,” published in the National Cathlic Bioethics Quarterly, Autumn 2006, by the National Catholic Bioethics Center:
“From a clinical standpoint, according to Dr. C. Ward Kischer, Ph.D., one of the leading authorities in the nation on human embryology, the abortion must be pre-arranged in order to have researchers available to immediately preserve the tissue.... ‘In order to sustain 95% of the cells, the live tissue would need to be preserved within 5 minutes of theabortion,’ stated Dr. Kischer. ‘Within an hour the cells would continue to deteriorate, rendering the specimens useless.’” p.11
(via Debra Vinnedge, quoting from her interview with Dr.Kischer at the American Life League conference, July 12, 2002; in Anthony Zimmerman,“Using Vaccines from Aborted Babies Makes Mephistophilus Laugh Again,” http://www.cogforlife.org/zimmerman.htm. Dr. Kischer is associate professor emeritus of cell biology and anatomy at the University of Arizona College of Medicine in Tucson.)
- The Institute of Medicine “Deliberations of the Human Fetal Tissue Transplantation Research Panel” discusses this ethical dilemma:
“The panel's report noted that ‘the reasons for terminating a pregnancy are complex, varied, and deeply personal’ and ‘regarded it highly unlikely that a woman would be encouraged to make this decision [to abort] because of the knowledge that the fetal remains might be used in research’...Defenders of the minority position argue, however, that knowledge of this possibility of benefit from the provision of fetal tissue would make a difference in some, perhaps even many, cases. Critics charge that HFTTR would reduce some pregnant women's ambivalence about abortion so that the possibility of an altruistic act—what could be called ‘general altruism’—would probably lead to some abortions that would not otherwise have occurred.”
“According to the panel, ‘the decision and consent to abort must precede discussion of the possible use of the fetal tissue and any request for such consent as might be required for that use,’ and ‘informed consent for an abortion should precede informed consent or even the preliminary information for tissue donation,’ except when the pregnant woman requests such information…Ideally the request and the decision to donate should follow the abortion decision itself, but because postmortem tissue deteriorates quickly and cryogenic storage is not possible for many transplants, ‘the pregnant woman must be consulted before the abortion is performed…”
Additional ethical dilemmas discussed:
- The Institute of Medicine “Deliberations of the Human Fetal Tissue Transplantation Research Panel” continues:
“Although the topic of societal legitimation tends to collapse into issues of complicity in and encouragement of abortions, it may be useful to consider it separately. According to Dorothy Vawter (1990), ‘to legitimate an act or practice is to justify or promote it in such a manner that others will become more inclined to regard it as acceptable and to engage in it.’ On the one hand, critics contend that federally funded HFTTR following elective abortions would tend to legitimate abortion because of the difficulty—or even the impossibility—of distinguishing within the expenditure of federal funds (1) approval of the use of fetal tissue from elective abortions and (2) approval of the elective abortions that produced the fetal tissue. Rabbi David Bleich argued in the panel's report that ‘[f]ederal funding conveys an unintended message of moral approval for every aspect of the research program.’”
“A second version of the societal legitimation argument focuses on society's acceptance of the benefits of human fetal tissue donations following elective abortions rather than on government funding. It would be difficult, perhaps even impossible, critics argue, for society to accept the benefits of HFTTR without becoming increasingly inclined to accept as legitimate the abortions that make the benefits possible. (Such a legitimation would be likely to occur even if no federal funds were used to support HFTTR protocols.) Thus, if HFTTR were to confer substantial benefits in the form of new life-saving or life-enhancing procedures, society would become less likely to delegitimate abortion by declaring many acts of abortion illegal (provided future Supreme Court decisions make such declarations more possible). It is not likely that society will renounce either the benefits of HFTTR or the decisions and practices that make the benefits possible.”
“A final criticism of societal legitimation appears in the panel's report in the dissenting letter by Daniel Robinson, who argued ‘that induced abortion is a moral wrong and that it cannot be redeemed by any actual or potential “good” secured by it. Thus, the possible medical benefits held out by research tissues obtained by such measures cannot be exculpatory’ (Robinson, 1988:73).”
“The fourth question posed by Assistant Secretary Windom was as follows: ‘Is maternal consent a sufficient condition for the use of the tissue, or should additional consent be obtained? If so, what should be the substance and who should be the source(s) of the consent, and what procedures should be implemented to obtain it?’ This question engendered one of the most divisive debates of the HFTTR panel as members wrestled with the problem of dispositional authority over fetal tissue following abortions, including the authority to transfer fetal tissue for use in transplantation research...The majority held that ‘fetal tissue from induced abortions should not be used in medical research without the prior consent of the pregnant woman. Her decision to donate fetal remains is sufficient for the use of tissue, unless the father objects (except in cases of incest or rape)’ (DHHS/NIH, 1988:60). Critics of this view contended that when the pregnant woman ‘resolves to destroy her offspring, she has abdicated her office and duty as the guardian of her offspring, and thereby forfeits her tutelary powers’ (Bopp and Burtchaell, 1988:47). From this perspective the abortion decision deprives the pregnant woman of any subsequent authority over the disposition of the fetus.”
“Affirming that there is no legal or ethical obligation to seek the father's permission, the panel nevertheless held that there is “a legal and ethical obligation not to use the tissue if it is known that he objects (unless the pregnancy resulted from rape or incest)” (DHHS/NIH, 1988:7).”
- It should be noted that many pro-life advocates would consider the lack of legal or ethical obligation in the protocol to seek the father’s permission a grievous breach of morality and a father’s rights.
Obviously these protocol did not exist when the initial cell strains used in vaccine development (WI-38 and MRC-5) were being developed, and we have no way of knowing what ethical standards those responsible for procuring the aborted babies used in their development imposed upon themselves. Additionally, we do know that at least one ethical guideline was breached in the development of the WALVAX-2 strain.
- “Brief History of Human Diploid Cell Strains” confirms that at least two aborted babies were specifically chosen for the development of cell strains to be used in vaccine production:
“WI-38 was obtained from a three-month-old female fetus:
‘This fetus was chosen by Dr. Sven Gard, specifically for this purpose. Both parents are known, and unfortunately for the story, they are married to each other, still alive and well, and living in Stockholm, presumably. The abortion was done because they felt they had too many children. There were no familial diseases in the history of either parent, and no history of cancer specifically in the families.’” p. 3
(via “Gamma Globulin Prophylaxis; Inactivated Rubella Virus; Production and Biologics Control of Live Attenuated Rubella Virus Vaccines” [no author given], American Journal of Diseases of Children 118.2 (August 1969): 377–278.)
“An article co-authored by Gard and colleagues at the Wistar Institute stated, in reference to Hayflick’s cell strains, that
‘ a human diploid cell strain derived from a fetal lung tissue was employed in-stead of monkey-kidney cells for the preparation of the attenuated poliovirus vaccine utilized in our study. The cell strain, cultivated especially for the production of virus vaccines, retains relatively constant morphology and chromo-somal characteristics…’” p. 3
(via J. S. Pagano et al., “The Response and the Lack of Spread in Swedish School Chil-dren Given an Attenuated Poliovirus Vaccine Prepared in a Human Diploid Cell Strain,”American Journal of Hygiene 79 (January 1964): 74–75.)
- According to the “Characteristics and viral propagation properties of a new human diploid cell line, walvax-2, and its suitability as a candidate cell substrate for vaccine production,” the established ethical protocol stating: “did not alter the timing, method, or procedures used to terminate the pregnancy solely for the purpose of obtaining the tissue for research…” cited in the “NIH Grants Policy Statement” per section 498A, was violated:
“The fetal material was provided by the Department of Obstetrics and Gynecology of Yunnan Hospital, with legal and ethical agreements from the donator. Before the study, we made strict and comprehensive inclusion criteria in order to guarantee a high quality cell strain: 1) gestational age 2 to 4 months; 2) induction of labor with the water bag method; 3) the parents career should not involve contact with chemicals and radiation; 4) both parents are in good health without neoplastic and genetic diseases, and with no history of human tissue or organ transplantation in the families traced for 3 generations; and 5) no infectious diseases. The tissues from the freshly aborted fetuses were immediately sent to the laboratory for the preparation of the cells.” (emphasis added on point number 2, mine)
- Nebraska Coalition for Ethical Research “The Ethics of the WALVAX-2 Cell Strain” identifies this as a breach of the aforementioned established ethical protocol:
“...the involved physicians performing the abortion should not deviate from the normal method of aborting the fetus (in the case of a three month fetus, a D&C) just so they might provide ‘optimal fetal tissue’ for the vaccine researchers. But this is what the doctors did in aborting the 3-month old female fetus whose tissue eventually proved to produce the best diploid cell strain out of the batch of 9 aborted fetuses for the Walvax-2 cell substrate. They employed a special means of induction (the water bag method) so they or someone they delegated, could deliver to Bo Ma et al intact fetal cadavers with fresh organs which would facilitate, in turn, the ready harvest of the needed fetal fibroblast lung tissue from which they developed the human diploid cell strain conducive to the growth of the respective viruses (rabies, hepatitis-A and varicella [chicken-pox]).”
A tangential, but highly relevant issue supporting the legitimacy of religious exemption from vaccination on pro-life grounds is the questionable safety of cell debris, DNA fragments, etc, from the aborted babies that are present in the final vaccine product administered to individuals. The presence of these materials and their uncertain safety status is well-attested in authoritative sources.
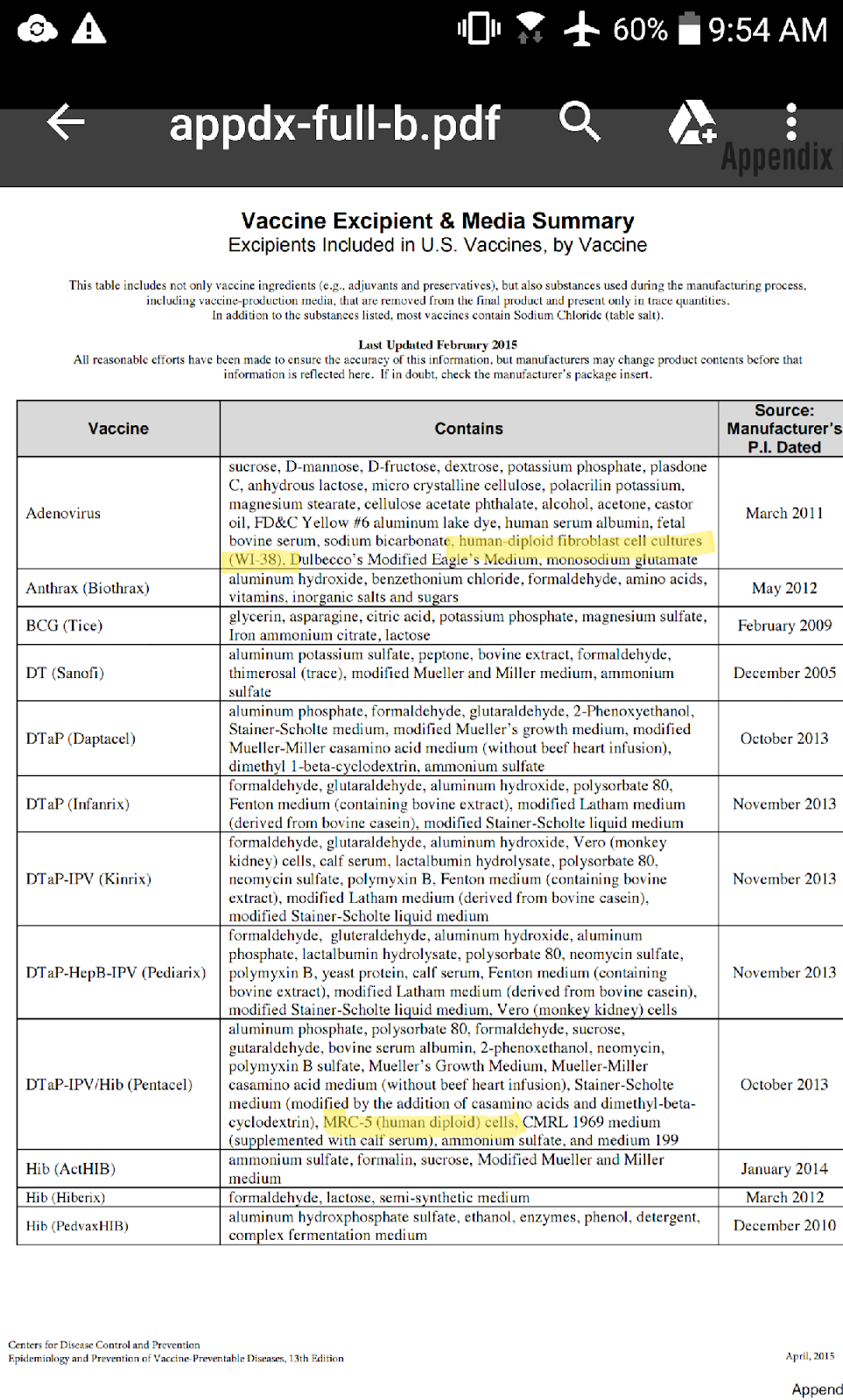
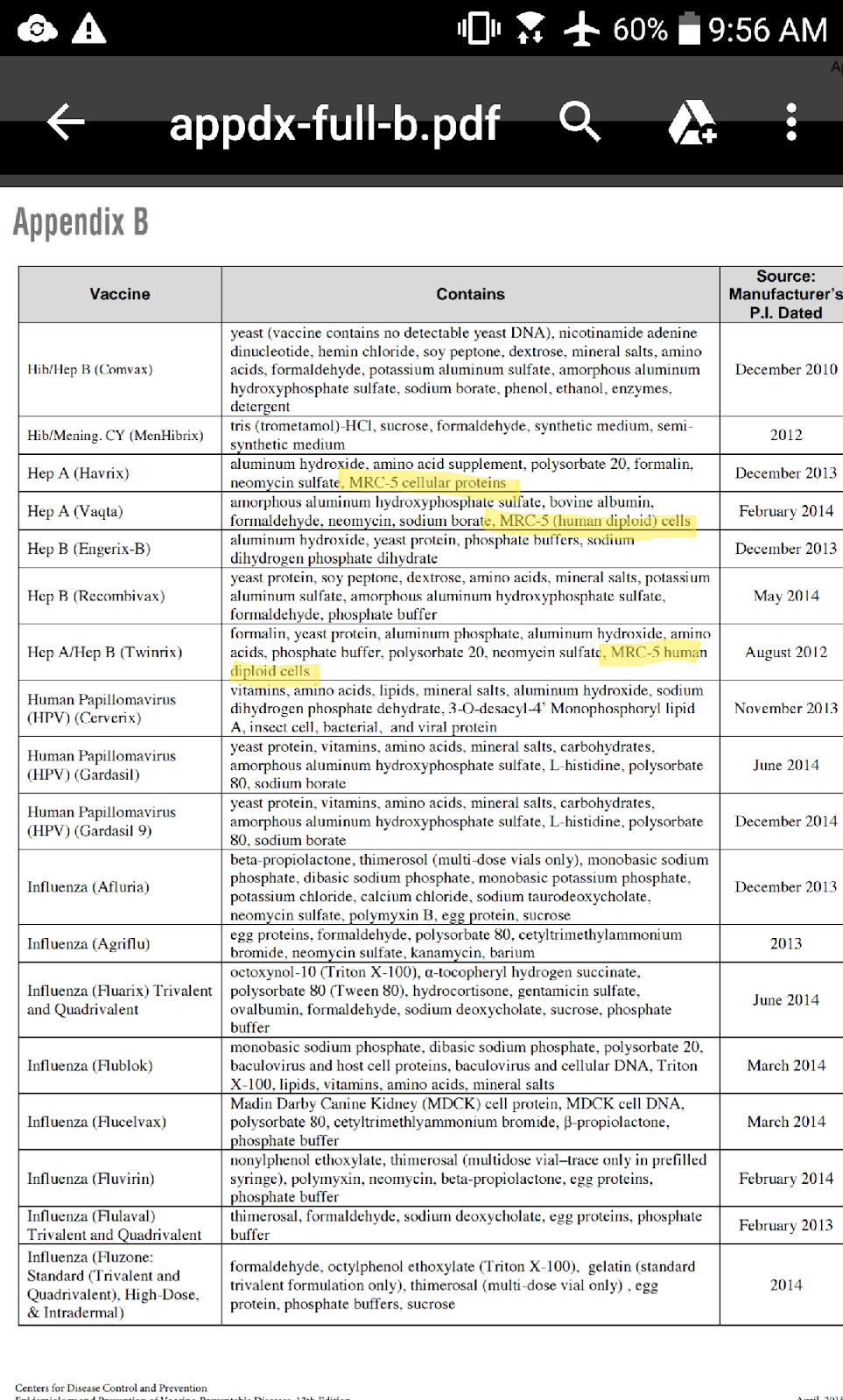
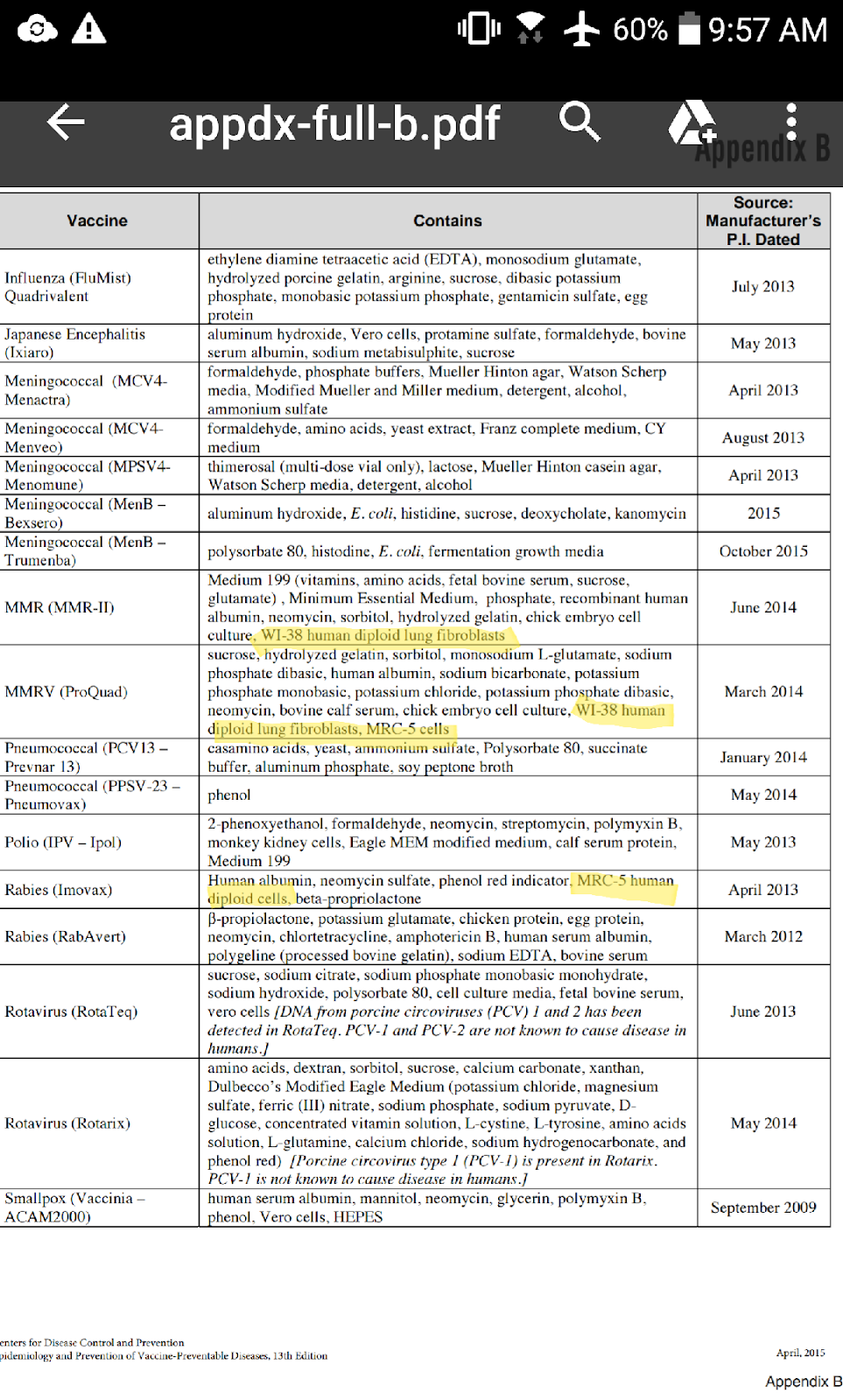
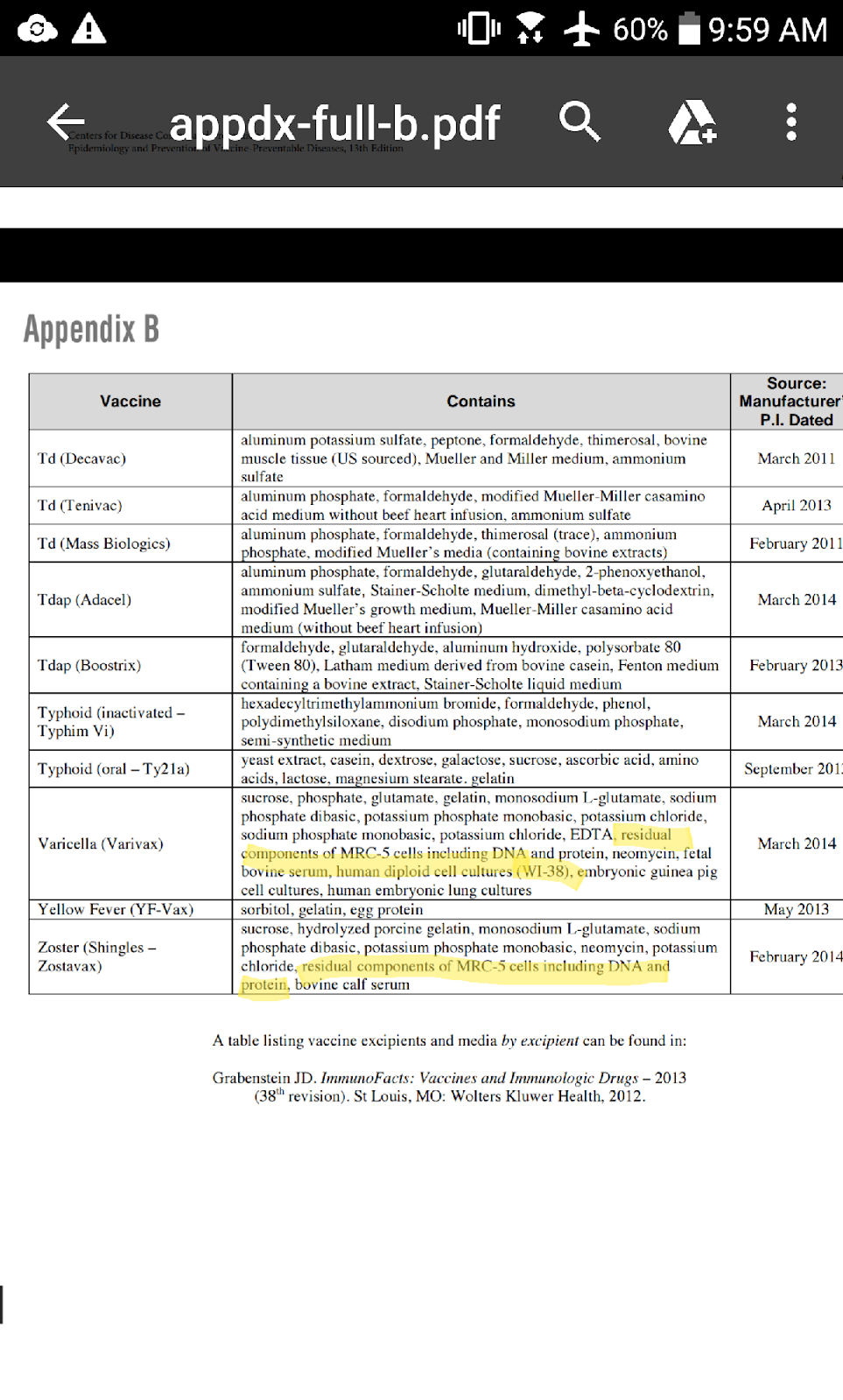
- The CDC Vaccine Excipient Summary (version updated January 2019) lists the following:
Hep A (Havrix): “MRC-5 cellular proteins…” p. 1
Hep A/Hep B (Twinrix): “MRC-5 human diploid cells…” p. 2
MMRV (ProQuad)(Frozen: Recombinant Albumin; MMRV (ProQuad)(Frozen: Human Serum Albumin); and MMRV (ProQuad)(Refrigerator Stable): “MRC-5 cells including DNA and protein…” p. 2
Varicella (Varivax)Frozen; Varicella (Varivax)Refrigerator Stable; Zoster (Shingles)(Zostavax) Frozen; and Zoster (Shingles)(Zostavax) Refrigerator Stable: “MRC-5 human diploid cells, including DNA & protein…”
- The CDC Vaccine Excipient Summary (version updated April 2015) listed WI-38 contents as well, which appears to have been removed from the version updated in 2019 linked above. There are other differences in the two lists relating to MRC-5, which I have not listed below. However, I have screenshots of the earlier version that I had taken and saved on my personal computer, which I will include as in Appendix A at the end of this document for comparison to the updated version linked above. The following is the WI-38 information omitted in the list above:
Adenovirus: “...human diploid fibroblast cell cultures (WI-38)...”
MMR (MMR II); MMRV (ProQuad): “...WI-38 human diploid lung fibroblasts…”
Varicella (Varivax): “...human diploid cell cultures (WI-38)...”
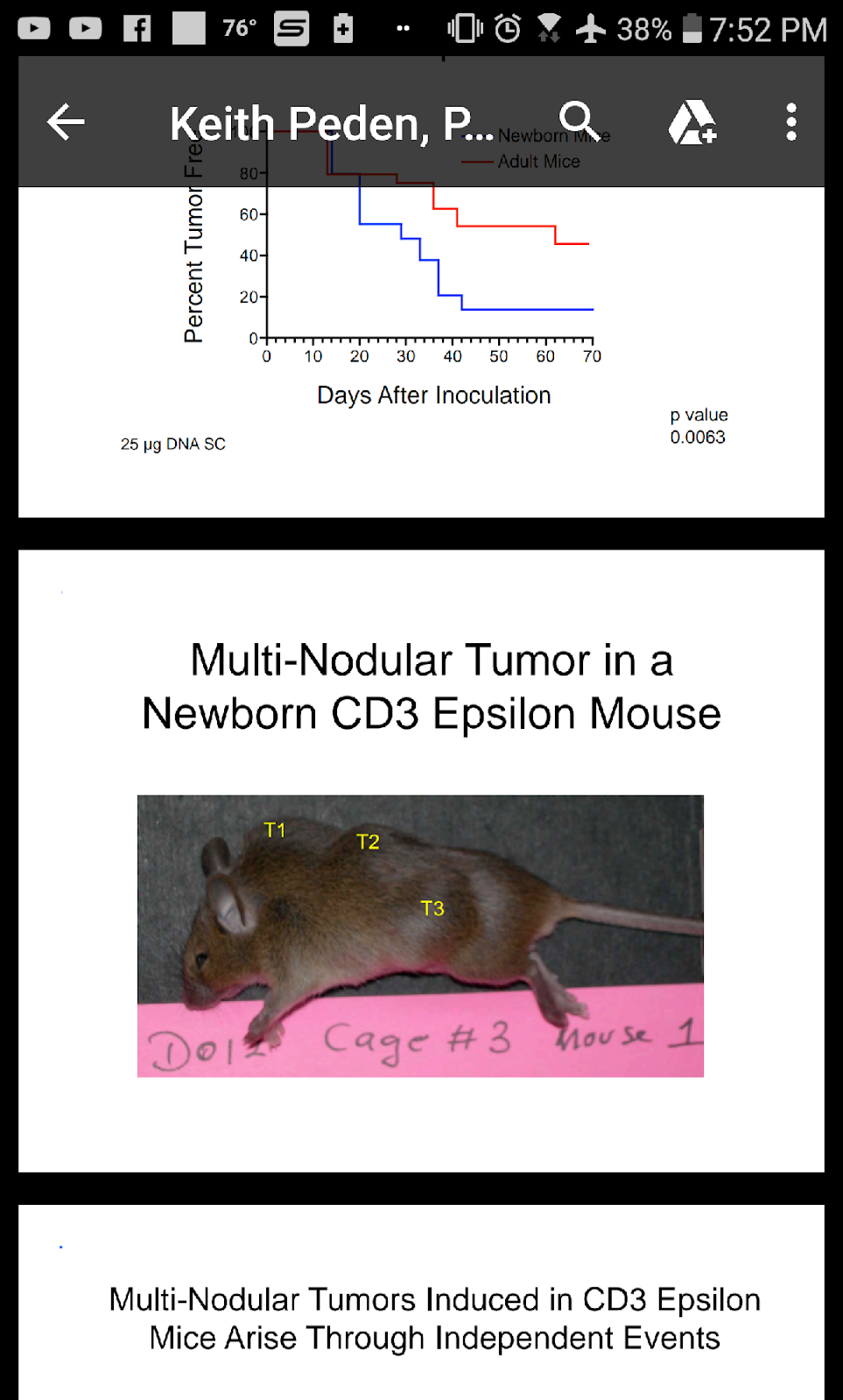
- The 2008 document, “Issues Associated with Residual Cell Substrate DNA: An Update,” authored by the FDA’s Keith Peden. I have included screenshots saved on my personal computer taken from Peden’s document, picturing the mice used for testing, which are included at the end of this document in Appendix B:
“Overall Aim of Our Studies To answer a 40 year-old question: Can residual DNA from the production cell substrate pose a risk to vaccine recipients?” p. 2
“Viral vaccines and biological products contain contaminating residual DNA from cell substrate...The amount of residual cell-substrate DNA in a vaccine will depend on the degree to which it can be purified…” p. 7
“Assessments Vary From: DNA is an ‘impurity’ whose amount needs to be measured but is not a safety concern To: DNA is a biologically active molecule whose activities pose a significant risk to vaccinees; thus, the amount of DNA needs to be limited and its activities reduced” p. 8
“Major Issues Associated with Residual Cell-Substrate DNA: Oncogenic Activity- Introduction of a dominant oncogene (e.g., ras), Infectivity Activity- Capacity to generate infectious agent (e.g., DNA virus, retroviral DNA)” p. 11
“Conclusions from DNA Oncogenicity: DNA appears to be more of an oncogenic risk than hitherto reported…” p. 45
“Issues Remaining to be Addressed: ...Contribution of the host immune system to DNA- induced tumor formation...Frequency of a DNA-induced initiation event...Whether hereditable epigenetic effects can induce oncogenic events in vaccine recipients and whether these could pose a safety concern” p. 48
- FDA: Vaccines, Blood and Biologics, “Investigating Viruses in Cells Used to Make Vaccines; and Evaluating the Potential Threat Posed by Transmission of Viruses to Humans”:
“The urgent demand for vaccines against emerging diseases has necessitated the use of novel cell substrates. These include tumorigenic cells such as MDCK and CHO cells (for influenza virus vaccines), 293 and PER.C6 cells (for adenovirus-vectored HIV-1 and other vaccines), and tumor-derived cells such as HeLa cells (for HIV-1 vaccines).” (cell lines derived from aborted babies italicized, my me, for emphasis)
“In some cases the cell lines that are used might be tumorigenic, that is, they form tumors when injected into rodents. Some of these tumor-forming cell lines may contain cancer-causing viruses that are not actively reproducing. Such viruses are hard to detect using standard methods. These latent, or ‘quiet,’ viruses pose a potential threat, since they might become active under vaccine manufacturing conditions.”
“The use of tumorigenic and tumor-derived cells is a major safety concern due to the potential presence of viruses such as retroviruses and oncogenic DNA viruses that could be associated with tumorigencity, Therefore, detection of persistent, latent DNA viruses, and endogenous retroviruses in vaccine cell substrates is important for vaccine safety, particularly in the development of live viral vaccines, where there are no or minimal virus inactivation and removal steps during vaccine manufacturing.”
- Section 13.1 of vaccine package inserts include a disclaimer for this safety issue. The following example is from the MMR II vaccine package insert:
“M-M-R II has not been evaluated for carcinogenic or mutagenic potential, or potential to impair fertility.” p. 6
“Observing vaccinated children for many years to look for long-term health conditions would not be practical, and withholding an effective vaccine from children while long-term studies are being done wouldn’t be ethical.”
Dr. Theresa Deisher’s work on the issues of safety surrounding the unacceptably high levels of human fetal DNA in the final vaccine product should especially be in the forefront of a pro-life/pro-science individual’s consideration. First, I will introduce Dr. Deisher, then I’ll cite her findings:
- Selected Excerpts from Dr. Theresa Deisher’s resume:
“PH.D., Department of Molecular and Cellular Physiology, Stanford University, Stanford, CA…”
“Post-Doctoral Fellowship, University of Washington,Department of Pathology/Hematology, Seattle, WA.,Dr. John Harlan”
“Dr. Theresa Deisher’s career has focused on discovering and developing new therapies for grievous human illness. Dr. Deisher obtained her PhD in Molecular and Cellular Physiology from Stanford University and has spent over 19 years in commercial biotechnology, working with such illustrious companies as Genentech, Repligen, ZymoGenetics, Immunex and Amgen, prior to founding AVMBiotechnology and Sound Choice Pharmaceutical Institute. AVMBiotechnology is the marquee prolife biotech company worldwide, certifying that it does not use morally illicit material in any process.”
“Dr. Deisher is an inventor on 23 issued US patents, and her discoveries have led to clinical trials of FGF18 for osteoarthritis and cartilage repair, and for Factor XIII for surgical bleeding. Dr. Deisher was the first person to discover adult cardiac derived stem cells, and has been a champion of adult stem cell research, both professionally and privately, for two decades. Dr. Deisher is a plaintiff in the US federal lawsuit to prohibit use of federal tax payer dollars for embryo destructive research. She is a frequent lecturer on the stem cell issues delving into topics such as; research, clinical progress, policy, economics and ethics…”
- Deisher and her colleagues published “Epidemiologic and Molecular Relationship Between Vaccine Manufacture and Autism Spectrum Disorder Prevalence.” in 2015:
“OBJECTIVES: To assess the public health consequences of fetal cell line manufactured vaccines that contain residual human fetal DNA fragments utilizing laboratory and ecological approaches including statistics, molecular biology and genomics.”
“Average single stranded DNA and double stranded DNA in Meruvax II were 142.05 ng/vial and 35.00 ng/vial respectively, and 276.00 ng/vial and 35.74 ng/vial in Havrix respectively. The size of the fetal DNA fragments in Meruvax II was approximately 215 base pairs. There was spontaneous and cellular and nuclear DNA uptake in HFF1 and NCCIT cells.”
“CONCLUSION: Vaccines manufactured in human fetal cell lines contain unacceptably high levels of fetal DNA fragment contaminants.The human genome naturally contains regions that are susceptible to double strand break formation and DNA insertional mutagenesis...”
- May 8, 2019, Dr. Deisher submitted the “Open Letter from Dr. Theresa Deisher to Legislators Regarding Fetal Cell DNA in Vaccines.” Excerpts follow:
“I am writing regarding unrefuted scientific facts about fetal DNA contaminants in the Measles-Mumps-Rubella vaccine, which must be made known to lawmakers and the public.”
“Merck’s MMR II vaccine (as well as the chickenpox, Pentacel ,and all Hep-A containing vaccines) is manufactured using human fetal cell lines and are heavily contaminated with human fetal DNA from the production process. Levels in our children can reach up to 5 ng/ml after vaccination, depending on the age, weight and blood volume of the child. That level is known to activate Toll-like receptor 9 (TLR9), which can cause autoimmune attacks.”
“To illustrate the autoimmune capability of very small amounts of fetal DNA, consider this: labor is triggered by fetal DNA from the baby that builds up in the mother’s bloodstream, triggering a massive immune rejection of the baby. This is labor.”
“It works like this: fetal DNA fragments[i] from a baby with about 300 base pairs in length are found in a pregnant mother’s serum. When they reach between 0.46– 5.08 ng/mL, they trigger labor via the TLR9 mechanism[ii]. The corresponding blood levels are 0.22 ng/ml and 3.12 ng/ml. The fetal DNA levels in a child after being injected with fetal-manufactured vaccines reach the same level that triggers autoimmune rejection of baby by mother.”
“If fetal DNA can trigger labor (a naturally desired autoimmune reaction), then those same levels in vaccines can trigger autoimmunity in a child. Fragmented fetal DNA contained in vaccines is of similar size, ~215 base pairs.[iii]”
“Administration of fragments of human fetal (primitive) non-self DNA to a child could generate an immune response that would also cross-react with the child’s own DNA, since the contaminating DNA could have sections of overlap very similar to the child’s own DNA.”
“Strong change-point correlation exists between rising autism rates and the vaccine manufacturing switch from animal-derived cell lines for rubella vaccine to human aborted cell lines in the late 70s[vi].”
“The earliest change point for Autistic Disorder (AD) birth year was identified for 1981 for California and U.S. data, preceded by a switch in the manufacturing process: In January 1979, the FDA approved the manufacturing switch for the rubella virus from animal based (high passage virus, HPV-77, grown e.g. in duck embryo cells) to the human fetal cell line WI-38 using the RA27/3 virus strain[vii]. Both the newly approved monovalent rubella vaccine and a trivalent mumps, measles and rubella vaccine utilize the WI-38 fetal cell line for manufacturing of the rubella vaccine portion.”
“The rubella portion of the MMR vaccine contains human derived fetal DNA contaminants of about 175 ngs, more than 10x over the recommended WHO threshold of 10 ng per vaccine dose[x].”
“Human endogenous retrovirus K (HERVK) is a contaminant in the measles/mumps/rubella vaccine[xiii]...Several autoimmune diseases have been associated with HERVK activity[xv]...The presence of both the high level contaminating fetal DNA as well as the HERVK contamination in the MMR vaccine is an unstudied risk with huge implications and dangers for individual and public health.”
“Solution: Pressure manufacturers to switch back to animal cell line derived rubella vaccines as was successfully done in Japan: Based on Takahashi strains of live attenuated rubella virus, produced on rabbit kidney cells. A single dose of this vaccine has been recently proven to retain immunity for at least 10 years when rubella was under regional control[xvii]. Split MMR vaccine into three individually offered options as done in Japan.”
Another moral and ethical complication driving the legitimacy of the religious exemption from vaccination on pro-life grounds is the fact that morally licit vaccine alternatives do exist that are not made available in the US. Pro-life religious organizations of all denominational stripes ubiquitously agree that pro-life/pro-vaccine individuals should opt for morally licit alternatives when available, and call for morally licit alternatives to be developed.
Specifically, recent outbreaks of measles in the US have prompted waves of legislation to remove the religious exemption from vaccination. However, the only measles vaccine available in the US, the MMR (measles, mumps, and rubella), is not morally licit. Ethical alternatives do, however, exist:
“Monovalent vaccines:.... Other vaccines containing non-Edmonston derived strains are also in use including Leningrad-16, Shanghai-191, CAM-70 and TD97. Most measles vaccines are produced in chick embryo cells, but few vaccines are grown in human diploid cells.” p. 1 (emphasis mine)
“More than ten live attenuated mumps vaccine strains (Jeryl Lynn, Urabe, Hoshino, Leningrad-3, L-Zagreb, Miyahara, Torii, NK M-46, S-12 and RIT 4385)have been used throughout the world...Several manufacturers in Japan and Europe produce a mumps vaccine containing the Urabe Am9 virus strain. However, concerns about vaccine-associated meningitis prompted several countries to stop using Urabe vaccine strain (WER 1992). Other vaccines have more limited distribution. In most cases, the viruses are cultured in chick embryo fibroblasts (such as for the Jeryl Lynn and Urabe strain-containing vaccines); however, quail and human embryo fibroblasts are also used for some vaccines.” p. 1 (emphasis mine)
“Most live attenuated rubella vaccines used throughout the world contain the RA 27/3 virus strain (Plotkin, 1965). Exceptions are vaccines produced in China (BRD2 virus strain) and Japan (Matsuba, Takahashi, and TO-336), produced on rabbit kidney cells, and the Matsuura strain, produced on quail embryo fibroblasts.” p. 1 (emphasis mine)
- The CDC’s “Q & A’s about Monovalent M-M-R vaccines” documents Merck’s decision not to resume production of three monovalent vaccine options, two of which, Attenuvax (measles), and Mumpsvax (mumps), are morally licit alternatives to MMR:
“On October 21, 2009, Merck announced that based on input from the Advisory Committee on Immunization Practices (ACIP), professional societies, scientific leaders, and customers, Merck has decided not to resume production of ATTENUVAX® (Measles Virus Vaccine Live), MUMPSVAX® (Mumps Virus Vaccine Live), and MERUVAX®II (Rubella Virus Vaccine Live).”
“ACIP recommends that ‘combined measles-mumps-rubella (MMR) vaccine generally should be used whenever any of its component vaccines is indicated.’ Receiving MMR vaccine rather than the separate component vaccines results in fewer shots and decreases the chance of delays in protection against all three diseases (measles, mumps and rubella). The AAP also recommends that combined MMR vaccine be used for immunization of U.S. children against measles, mumps, and rubella.”
“Persistence of Immunity Acquired after a Single Dose of Rubella Vaccine in Japan.” discusses a morally licit alternative to the Rubella vaccine:
“To date, Takahashi, Matsuura, and TO-336 strains of live-attenuated rubella vaccine have been used in Japan. Japan implemented a single-dose rubella vaccination program until 2006. However, few reports are available on the persistence of immunity after this vaccination program. We collected 276 serum samples from January 2009 to December 2011 at Okafuji Pediatric Clinic and assessed the immune status of these samples against rubella virus during 1-10 years after vaccination with a single dose of Takahashi rubella vaccine. Regional outbreak of rubella did not occur during 1999-2011...Our results showed that all the tested serum samples contained antibodies against the rubella virus 10 years after the vaccination.”
Other vaccines for which morally licit alternatives exist are Hepatitis A, Polio, Rabies, Shingles, Rheumatoid Arthritis, and Smallpox (*NOTE* some of these vaccines are currently available in the US, and some are even given preference over the morally illicit alternative):
“Immunogenicity of aluminum-adsorbed hepatitis A vaccine (Havrix®) administered as a third dose after primary doses of Japanese aluminum-free hepatitis A vaccine (Aimmugen®) for Japanese travelers to endemic countries.” mentions Aimmugen, which is a Japanese morally licit Hepatitis A vaccine alternative:
“...only one licensed hepatitis A vaccine is available in Japan. This vaccine is a lyophilized inactivated aluminum-free hepatitis A vaccine (Aimmugen®)...Aimmugen® is not available in countries other than Japan.”
- The CDC’s “Polio Vaccine Composition, Dosage, and Administration” states:
“Two inactivated polio vaccine (IPV) products are licensed in the United States. However, only IPOL® is still used in the United States.” (** IPOL is morally licit)
“Some combination vaccines (several different vaccines in the same shot) contain IPV, such as Pentacel (DTaP-IPV/Hib), Pediarix (DTaP-IPV-HepB), or Kinrix (DTaP-IPV).” (** Pentacel is not morally licit; Pediarix is morally licit)
- FDA vaccine package insert for the morally licit RabAvert rabies vaccine:
“RabAvert Rabies Vaccine produced by GlaxoSmithKline GmbH is a sterile, freeze-dried vaccine obtained by growing the fixed-virus strain Flury Low Egg Passage ( LEP) in primary cultures of chicken fibroblasts.”
- CDC’s “Shingles Vaccination” page:
“Two vaccines are licensed and recommended to prevent shingles in the U.S.. Zoster vaccine live (ZVL, Zostavax) has been in use since 2006. Recombinant zoster vaccine (RZV, Shingrix), has been in use since 2017 and is recommended by ACIP as the preferred shingles vaccine.” (**Shingrix is morally licit)
- FDA Medication Guide Humira (rheumatoid arthritis):
“To reduce the signs and symptoms of: moderate to severe rheumatoid arthritis (RA) in adults...moderate to severe polyarticular juvenile idiopathic arthritis (JIA) in children 4 years and older…”
- CDC’s Smallpox page ACAM2000:
“The Strategic National Stockpile (SNS) has three smallpox vaccines: ACAM2000® – the only licensed smallpox vaccine in the United States”
See next page for Appendix A
APPENDIX A
Screenshots saved on my personal computer of the CDC Vaccine Excipient and Media Summary last updated April 2015, including information omitted from the list updated January 2019:
Appendix B
Screenshots saved on my personal computer of the FDA document “Issues Associated with Residual Cell Substrate DNA: An Update,”: