We have very little data on the use of menopause hormone therapy after age 65, so it was exciting to have a new paper that specifically looks at this age group. As the study provided much information, I addressed the estrogen-only aspect in the previous post (located here). Today, I will discuss the estrogen plus progestogen arm, also known as combination therapy.
One very important note. Most women using menopause hormone therapy take the type of regimen we are about to discuss, an estrogen plus progestogen. Unfortunately, some people primarily use the estrogen-only findings to talk about all menopause hormone therapy. This serves no one, as they are different regimens. Okay, maybe it serves people who have built a career around hormones solving everything. But that isn’t what happens here because you deserve facts.
Just a reminder, this is an observational study, so cause and effect can’t generally be inferred. For example, in this study, low-dose vaginal estrogen, products that do not raise the estrogen level above the menopausal range, reduced the risk of lung cancer by 19% and colon cancer by 20% (both results were statistically significant), but medium doses of vaginal estrogen (estrogen meant to be absorbed) did not have this effect. This seems biologically implausible and is likely a statistical artifact.
With any observational study, it’s important to consider the findings in context and be careful about projecting what we may or may not want the results to be.
Okay, let’s get into it.
Brief Intro
The study is a database review of electronic medical records from the US Centers for Medicare and Medicaid Services (CMS). The researchers looked at who received hormones and who didn’t and also evaluated a variety of important health outcomes: death, five different types of cancer (breast, lung, endometrial, colon, and ovary), cardiovascular disease (six different types, including stroke and blood clots), and dementia. A medium or standard dose of hormones was 0.625 of conjugated equine estrogens (CEE or Premarin), 1 mg of oral estradiol, 5 μg of oral ethinyl estradiol, a transdermal 50 μg patch, and a vaginal delivery of 50 μg estradiol. Women were not randomly assigned to hormones or a placebo, so many unknown variables exist.
There were many permutations and combinations of regimens. In addition, the grouping of some of the results in the paper could be confusing or misleading. For example, the oral estrogen plus progesterone or oral estrogen plus progestin categories both include estradiol and Premarin (conjugated equine estrogens or CEE). However, they are not the same hormones, and Premarin is not a major player in the menopause therapy market right now (outside of Duavee, and there is no data here on that drug combination). Premarin could give different results than estradiol, so they should really be looked at separately. Another example is the weird grouping of low-dose estrogen, which includes both low-dose vaginal estradiol (a product meant to stay in the vagina and not cause estradiol levels to rise over that seen in the menopause range) and low-dose transdermal estradiol meant to enter the blood and raise the levels. Therefore, I decided to dive into the supplemental data and gather information on the most common regimens. This means I focused on transdermal estradiol and oral estradiol regimens with either progesterone or a progestin. If you need a refresher on progesterone vs. progestins, read this post.
The following few sections will be pretty in-depth, so like my previous post on this topic, you can keep reading (and I don’t mean to discourage you from that) or skip to the “Putting it All Together” section if you feel your eyes glazing over.
Mortality and Cancer Risk
I created a table showing some of the key findings with the most common regimens used today. The findings represent the increased or decreased risk associated with the hormone regimens as compared to women over 65 not taking hormones. Hopefully, this provides a quick and easy way to look at the data. Results that were not statistically significant are in black type and have NS below the number (basically, consider these results as no change in risk). Numbers with a positive value mean an increased risk (bad) and are also highlighted in red. And, of course, numbers with a negative value mean a reduced risk (good) and are in green text. Values with an asterisk have a stronger statistical signal.
Table 1: Overall Mortality and Risk of Breast, Lung, Endometrial, Colon and Ovarian Cancer with Combined MHT
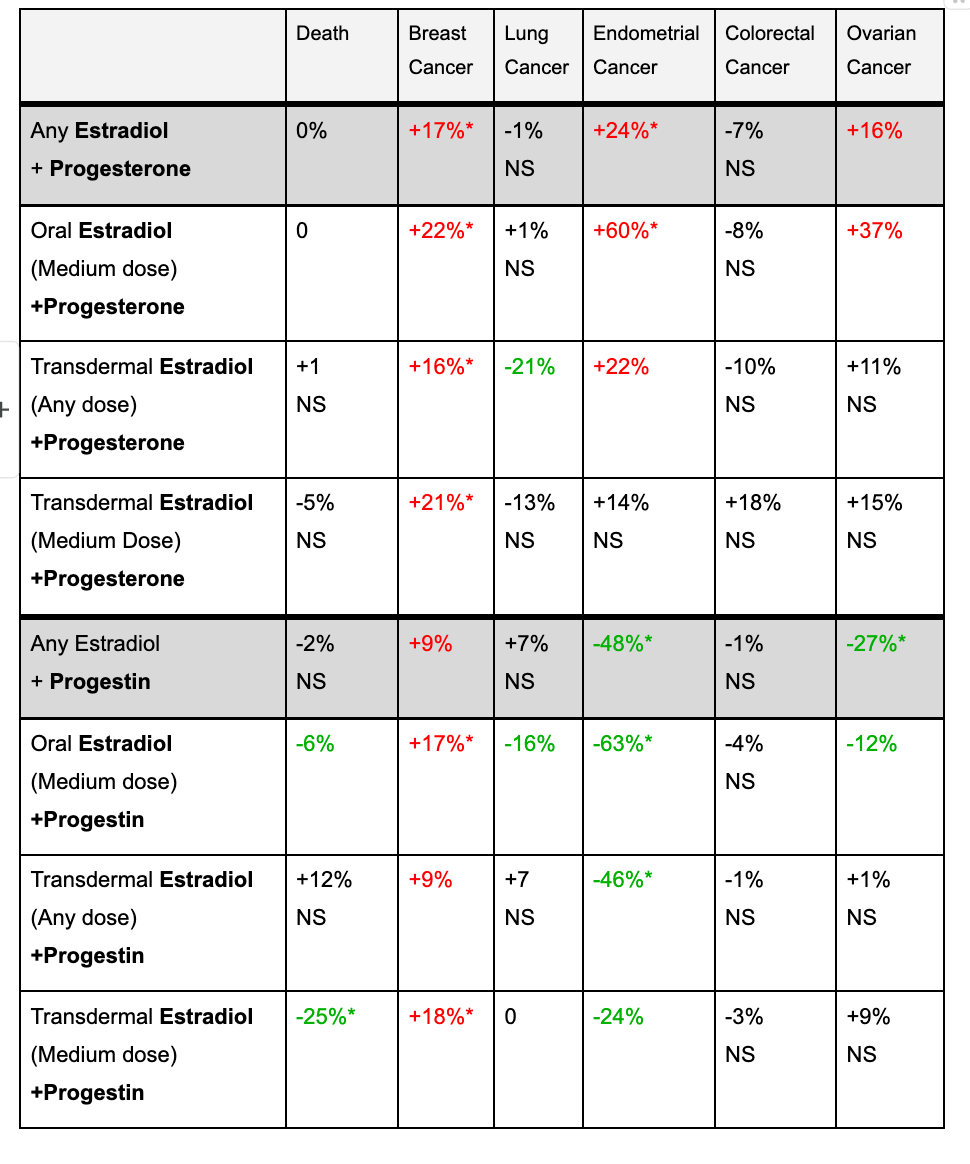
I’m going to exclude colon cancer from the analysis. As you can see, looking down that column, none of the results are statistically significant. The lung cancer and ovarian data are also a little challenging, with the results being somewhat all over the place. So, let’s focus on overall mortality, breast cancer, and endometrial cancer.
Mortality
Look at the far left column, which is mortality. The only real standout for reducing mortality is progestin combined with a medium dose of oral or transdermal estradiol (transdermal having the stronger effect). Whether this is an artifact, meaning the study couldn’t account for other differences, a statistical snafu, or a true effect is impossible to know. If we look closer at the transdermal data, which has the strongest signal, we only see a reduction in mortality with the medium dose of progestin. The idea that only a medium dose of transdermal estradiol with a progestin is associated with a lower mortality, but none of the other transdermal regimens, is either an extraordinary finding or it’s not a real finding.
My takeaway regarding mortality is there is no negative safety signal. This is a good thing!
Cancer
For breast cancer, both the progesterone and progestin regimens were associated with an increased risk. There was a trend for the lowest doses of transdermal and oral estradiol, with either progestin or progesterone, to have less of an effect or even no increased risk.
We know from other observational studies that MHT with progestins/progesterone is associated with an increased risk of breast cancer. Most other observational data suggest that progestins have a higher risk, but in this study, progesterone was more likely to be associated with a higher risk of breast cancer. I think this points out the inadequacies of observational studies. So, the best we can say is the increased risk of breast cancer with combination MHT appears to persist past age 65, which is what other observational studies have shown, and maybe with combination therapy, the risk is less with lower doses of estrogen. I know there will be lots of questions about breast cancer, and I will be writing about that in more detail in a follow-up post.
The conclusion from this study is that breast cancer risk is increased (not a new finding), and maybe we need to take a closer look at breast cancer risk for progesterone vs. progestins.
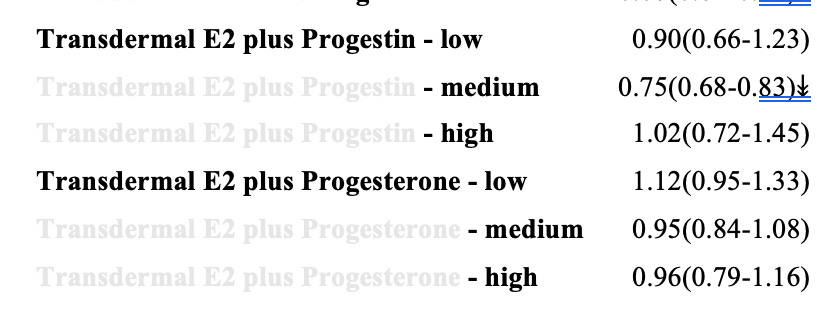
The endometrial cancer data is interesting. Below is the information from the supplement, with the nonrelevant columns and rows removed. You can see that progestins are generally associated with much lower rates of endometrial cancer than progesterone. In fact, the risks are higher for some of the progesterone-based regimens. (A number less than one means a lower risk, and two arrows, either up or down, signifies a stronger statistical finding).
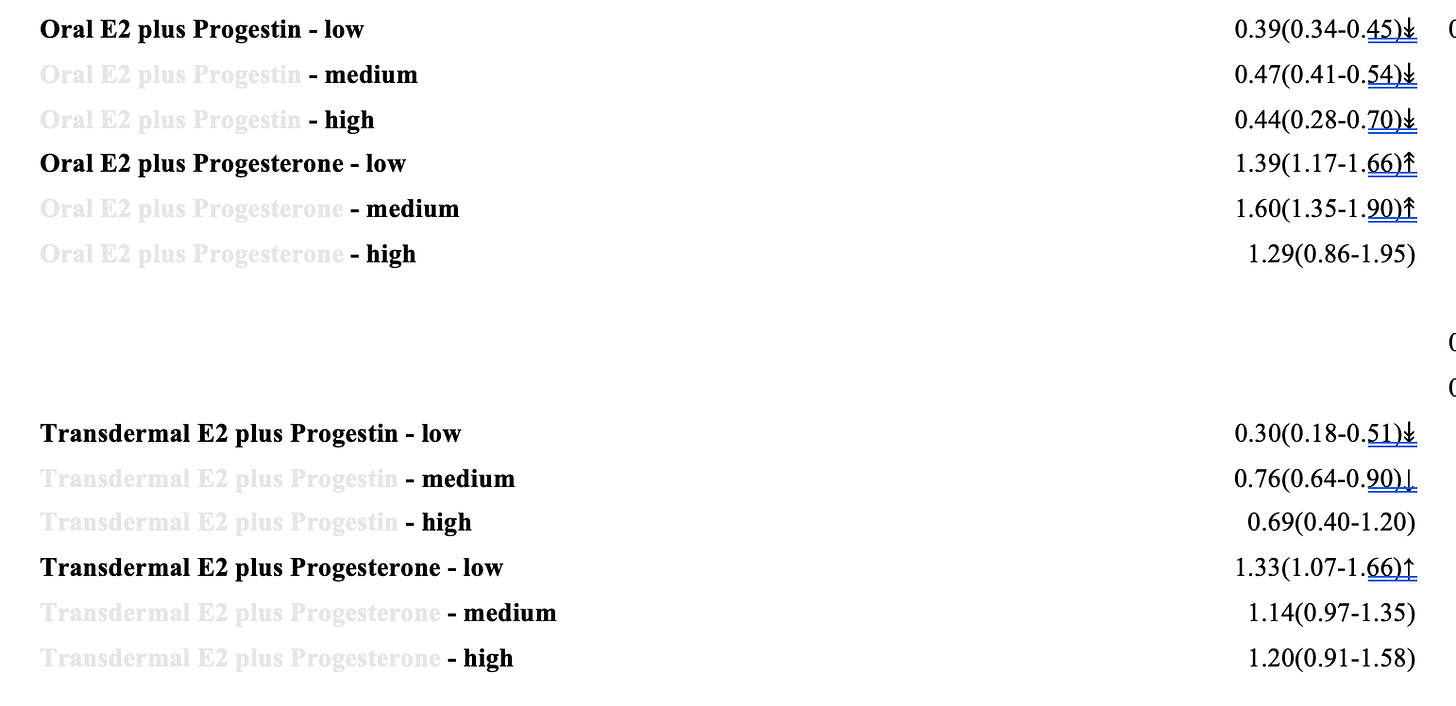
Progestins performing better at preventing endometrial cancer isn’t surprising, because we know they are better at suppressing estrogen's negative effect on the endometrium than progesterone, but the magnitude of the difference between the two was a little surprising.
The best we can say here is there is a safety signal about progesterone being adequate to suppress the endometrium vs. progestins in MHT. This shouldn’t alarm anyone. We need more data here, so a conclusion isn’t possible. However, for someone at high risk for endometrial cancer, this study does support considering a progestin over progesterone to protect the endometrium.
Cardiovascular Disease
The researchers evaluated six different kinds of heart disease: ischemic heart disease (IHD), congestive heart failure (CHF), blood clots (VTE), stroke, atrial fibrillation (AF), and heart attack (AMI).
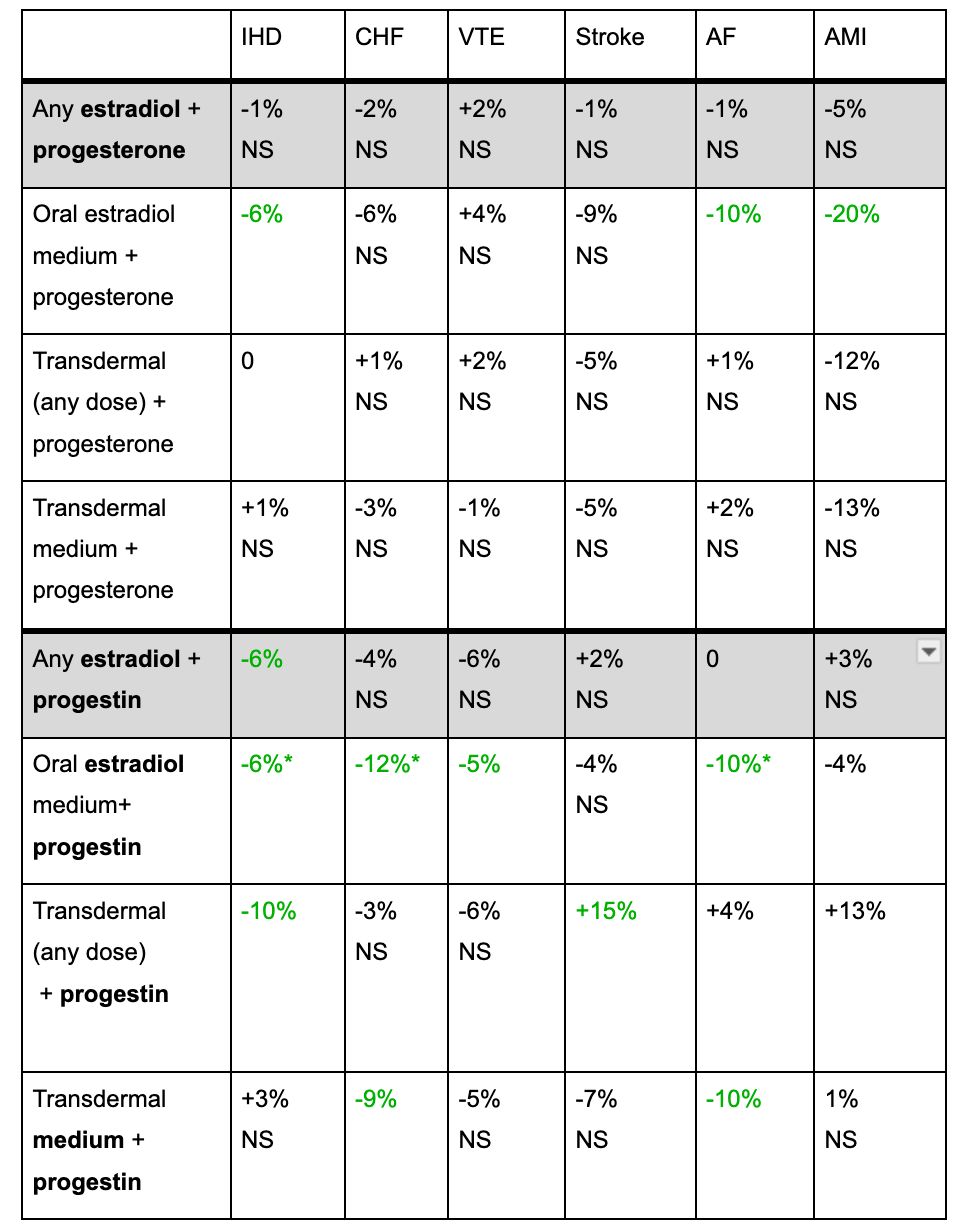
The most reassuring thing is that there were no negative signals, which is a big takeaway. As for protecting the heart, there was a statistically significant improvement in some domains, but it wasn’t very consistent across the dosing, and overall, it’s hard to say MHT is cardioprotective from this data. Interestingly, progestins seemed to perform better than progesterone.
Dementia
Only a low dose of oral estradiol plus progestin was associated with a statistically significant reduction in dementia (12%); otherwise, it was neutral across the board. This also means there is no support here for combined MHT past age 65 reducing dementia.
Putting it All Together
In this study, combination estrogen therapy after age 65 was not associated with an increased risk of mortality, colon cancer, cardiovascular disease, or dementia. These are important takeaways. This study doesn’t support combined MHT reducing the risk of dementia or the progesterone-based regimens protecting the heart. The data for the progestin-based regimens protecting the heart was a bit all over the place.
Overall, progestin regimens tended to perform better in several domains, which is surprising given the findings of other observational studies.
There was, as expected, an increased risk of breast cancer, more so with progesterone vs progestin regimens, which has not been shown in other observational data. Until now, the data suggested progesterone has a lower risk of breast cancer. The lowest dose of transdermal estradiol wasn’t linked with an increased risk of breast cancer, but whether that is a true effect or not isn’t possible to know.
Progestins were more protective than progesterone for endometrial cancer, and I think this is one of the more important findings. I think this needs further study and might be something for someone at high risk for endometrial cancer to consider when thinking about MHT.
The authors concluded that estrogen plus progestin “exhibited risk reductions in endometrial and ovarian cancers, ischemic heart disease, congestive heart failure, and venous thromboembolism.” In contrast, estrogen plus progesterone “exhibited risk reduction only in congestive heart failure.”
For those who want to continue MHT past age 65, as long as they are aware of the increased risk of breast cancer and aware that there may be some unanswered questions about progestin vs. progesterone, there is no reason to say they shouldn’t, given the mortality data is neutral and that they understand this is based on observational data.
References
Baik, SH, Baye F, McDonald CJ. Use of menopausal hormone therapy beyond age 65 years and its effects on women's health outcomes by types, routes, and dosesMenopause ():10.1097/GME.0000000000002335, April 9, 2024. | DOI: 10.1097/GME.0000000000002335
NAMS Position Statement. The 2022 Hormone Therapy Position Statement of The North American Menopause Society. Menopause. 2022;29:767-794.
Cynthia A. Stuenkel et al. Treatment of Symptoms of the Menopause: An Endocrine Society Clinical Practice Guideline, The Journal of Clinical Endocrinology & Metabolism, Volume 100, Issue 11, 1 November 2015, Pages 3975–4011, https://doi.org/10.1210/jc.2015-2236.
Asi, N., Mohammed, K., Haydour, Q. et al. Progesterone vs. synthetic progestins and the risk of breast cancer: a systematic review and meta-analysis. Syst Rev 5, 121 (2016). https://doi.org/10.1186/s13643-016-0294-5
Collaborative Group on Hormonal Factors in Breast Cancer. Menarche, menopause, and breast cancer risk: individual participant meta-analysis, including 118 964 women with breast cancer from 117 epidemiological studies. Lancet Oncol. 2012;13(11):1141–1151.
Santen RJ, Heitjan DF, Gompel A, et al. Underlying Breast Cancer Risk and Menopausal Hormone Therapy, The Journal of Clinical Endocrinology & Metabolism, Volume 105, Issue 6, June 2020, Pages e2299–e2307,