Table of Contents
2.1 Visual Map of Lived Experiences 3
2.2.2 Underlying Structures and Mental Models 6
2.2.3 Data on Income, Race, and Access to Full-Service Grocery Stores 9
3. Systems Thinking Approach 10
3.2 Stakeholders & Solutions Map 11
4. Stakeholders and Solutions 12
4.2 Educational Institutions 13
4.7 Existing Global Solutions 18
4.7.1 World Food Programme (WFP)’s Fresh Food Voucher (FFV) Programme in Ethiopia’s Amhara Region 18
4.7.2 Participatory Urban Agriculture Program (AGRUPAR) in Quito, Ecuador 18
4.8 Insights and Takeaways: Stakeholders and Solutions 19
5. Recommendations, Key Insights, and Lessons Learned 21
5.2 Centering the Agency, Identity, and Humanity of Communities 21
5.3 Cross-Sector Collaboration 23
5.4 Invest in Public Transportation Infrastructure 24
1. Introduction
Food access is a pressing systemic issue in Washington D.C. in Wards 7 and 8, whose residents are primarily from low-income Black and Brown communities (Smith, 2021). Food insecurity extends beyond daily barriers to getting food every day—from the lack of healthy food options at nearby convenience stores to the severe inequality of grocery store distributions in these communities that contributes to food apartheid. This problem is exacerbated by discriminatory urban planning practices, a lack of affordable housing, and rapid gentrification which pushes residents out of central parts of D.C. to Wards 7 and 8 and contributes to generational social and racial equity issues. Inefficient government actions that do not center community input and the fixation on profit-based models by corporations and governments also perpetuate these issues, along with many stigmas surrounding residents of Wards 7 and 8 regarding welfare programs and poverty. Community-centered approaches by residents and non-profit organizations have the power to address the systemic roots of barriers to food access in Wards 7 and 8 but need to be prioritized to effectively address this issue.
2. Challenge Landscape
2.1 Visual Map of Lived Experiences

2.2 Iceberg Model
2.2.1 Events and Patterns
Events | Patterns and Trends | |
The Grocery Gap & lack of incentives for supermarkets | More than ¾ of the city's food deserts are in Wards 7 and 8 (Smith, 2021), with half in Ward 8. | Grocers flock to areas they believe they can make a profit, but there is a lack of financial incentives to locate in poor communities (Watson, 2018). As of 2021, Ward 8, the lowest-income ward in DC, contains one full-service grocery store for every 85,160 residents; contrastingly, Ward 3, the highest-income ward, has one full-service grocery store for every 9,336 residents (Anacostia Community Museum). As a result, the fundamental demand for fresh foods is not being met by available markets, many of which are convenience stores that lack healthy options. |
Income, unemployment, and access to food. | Transportation is significantly more difficult to access in Wards 7 and 8, posing a further challenge to accessing healthy food (Jensen et al., 2020). Convenience stores and other existing food providers in Wards 7 and 8 typically lack culturally appropriate food catered to the diets and traditions of residents. | More than 40% of households in Wards 1, 2, and 8 do not own a car (Smith, 2021). With higher incomes, families are more likely to be able to afford alternative means of private transportation such as Ubers or Taxis to reduce travel time; however, with lower median incomes, it is unlikely that families are able to minimize travel time when shopping for groceries. As a result, lower-income households commonly face transportation barriers to accessing food. Despite D.C.’s relatively high overall walkability score of 76, Wards 5, 7, and 8 all have scores that merely match the description of being “somewhat walkable” (Jensen et al., 2020). Moreover, with only two stations on the Washington Metropolitan Area Transit Authority (WMATA) Metrorail lines in Ward 8 and three in Ward 7, Wards 7 and 8 have two of the lowest median transit scores in D.C. (Jensen et al., 2020). |
Disparate health outcomes | Wards 7 and 8 have significantly worse health outcomes. | Higher percentages of populations in Wards 7 and 8 suffer from diet-related diseases and self-reported poor health (Jensen et al., 2020). Additionally, nearly three-fourths of the population in Wards 7 and 8 are considered overweight or obese, contributing to the low life expectancies of 72, compared with the average life expectancy of 88 for a person living in Ward 3 (Jensen et al., 2020). These high rates of diet-related disease are exacerbated by the lack of access to fresh, nutritious food. The health conditions also make individuals more susceptible to health risks such as COVID-19; residents in Wards 7 and 8 have suffered the highest COVID-19 death rates per capita compared to any other ward (Jensen et al., 2020). The emotional toll that budgeting for grocery shopping along with other essential needs for low-income households contributes to mental health issues, affecting overall wellbeing (Jensen et al., 2020). As a result, these combined health detriments also contribute to poor performance at work and school (Chilton & Rose, 2009), ultimately impairing national productivity. |
Lack of systemic solutions | Many organizations focus on food donation models or systems that provide food directly instead of addressing other issues related to food access. | Even with the presence of community-based food programs such as Healthy Corners, farmers’ markets, and community gardens, there is still a fundamental lack of sufficient and reliable access to healthy and affordable food (Jensen et al., 2020). There are new full-service grocery stores being built in both Wards 7 and 8; however, this will not single-handedly reverse the current trend; the grocery gap and food insecurity rates across the city remain very high (Jensen et al., 2020). |
The identities of people who struggle with food insecurity, systemic racism, and affordable housing | Majority Black and Brown communities in Wards 7 and 8 have been displaced from wealthier parts of the city. Public housing projects are concentrated in Wards 7 and 8 (Socialserve, 2022). | Rising costs of living lead to white flight but leave marginalized communities no choice but to remain in poorer resourced communities. |
Schools and food accessibility | High rates of free and reduced lunch for students in Wards 7 and 8. Free and reduced lunch programs are key to meeting the nutritional needs of Title 1 eligible students, but only provide meals during the week (District of Columbia Public Schools, 2022). | Heavy community reliance on free lunches from schools to provide basic nutritional needs for students, especially with rising food insecurity due to income inequity and the COVID-19 pandemic. |
2.2.2 Underlying Structures and Mental Models
Underlying Structures | Mental Models | |
The Grocery Gap and lack of incentive for supermarkets | Because wealthier residents leave Wards 7 and 8 to work in other parts of the city, the lack of concentrations of office buildings and other profitable amenities makes it unappealing for grocers to open in these poorer communities. For example, Walmart previously committed to opening a store in Ward 7, but they eventually revoked this agreement, citing “profitability concerns” (Watson, 2018). Factors that influence the profitability of the store location include the neighborhood’s median household incomes, education level, and homeownership (Jensen et al., 2020)—all of which relate to historical obstacles excluding Black and Brown communities. The consequence is a disproportionate prevalence of food apartheid in Wards 7 and 8 due to race and socioeconomic status (Jensen et al., 2020). | Stereotypes that communities don’t care about eating healthy food (Reichler). |
Income, unemployment, and access to food. | Lack of efficient channels of communication and outreach with communities in a sensitive way to inform them of initiatives to improve nutritional quality and access (Reichler). This relates to a lack of community input in policies and initiatives to address their needs, which diminishes the effectiveness of these programs. While D.C. is not necessarily a driver-friendly city, public transit remains significantly inaccessible to lower-income populations. These obstacles hinder communities from obtaining fresh and nutritious food. As a result, these communities have no choice but to turn to convenience stores that mostly serve processed, nonperishable foods which can be detrimental to their health (Jensen et al., 2020). The difficulty of accessing credit for small businesses makes it difficult for local businesses to thrive in Wards 7 and 8 and for community members to work towards economic mobility through entrepreneurship. This contributes to the increasing racial wealth gap in D.C. (Jensen et al., 2020). | Stigmas around using food stamps and welfare programs pose barriers to accepting federal assistance. The concept of a “welfare queen” (Anacostia Community Museum) and ideas that welfare expansion programs are not necessary. The perception that public transportation is only used by “poor” people (Janette Sadik-Khan, 2020), with other means of travel designed to serve wealthier communities. Disregarding cultural differences in food preference, utilization, and language framing contribute to a lack of culturally competent food options. |
Disparate health outcomes | Geographic isolation of marginalized communities from hospitals and other health centers, disparities in insurance access, and lack of nutrition education contribute to generational, community-wide health disparities (Chan, 2020). | The lack of adequate nutritional education leads to the perception of food as a source of calories instead of nutrition. |
Lack of systemic solutions | Shortfalls of government efforts to provide for people’s needs and the intentional exclusion of marginalized communities from Great-Depression-era welfare programs like the initial rollout of food stamps and loans for small businesses that were restricted to white Americans. Industrialization of the food system and supply chains contributes to dependence on large grocers and a lack of knowledge and interest in independently growing food. The commodification of food and fixation on profit as opposed to valuing the idea of food as a right shifts priorities away from addressing food sovereignty. | Viewing food insecurity as an isolated issue just about food (Reichler), and advocating for solutions without considering the role of food sovereignty. Viewing food as a commodity instead of a right. Ignoring the influence of structural racism and classism, and the lasting effects of intentional exclusion of low-income and Black and Brown communities. A “savior” mindset that excludes community members when developing initiatives. Solely connecting food issues and access to geographical location; using the term “food desert” as opposed to “food apartheid”—which more holistically encompasses the oppressive and structural dynamics which lead to inequalities in the food system (George & Tomer, 2021). Rather than simply geographic location, grocery store placement is influenced by systematic racism: The Black/White race segregation of 62.3 (highly segregated) based on the 2010 Census reflects the continued socioeconomic disparities between majority Black vs. majority White wards in accessing food (Jensen et al., 2020). |
The identities of people who struggle with food insecurity, systemic racism, and affordable housing | Black and Brown communities were intentionally segregated through redlining practices in the 1930s. As other parts of D.C. were developed, these communities remained underserved and underinvested. Gentrification and a lack of affordable housing in Central and Northwest parts of D.C. pushed out lower-income primarily Black Washingtonians to Wards 7 and 8 where housing was more affordable, but resources like grocery stores continue to be severely lacking. The racial wealth gap represents the disparity between White and Black Americans’ ability to build and maintain wealth as a result of historically racist policies and laws (Jensen et al., 2020). The laws of redlining, the denial of loans and credit, and being excluded from higher education and white-collar jobs all contribute to the present effects of disparity between White and Black family incomes. As the only wards in D.C. with a majority Black population, Wards 5, 7, and 8 also have the highest percentage of unemployment, lowest median incomes, smallest growth in income, and highest rates of poverty (Jensen et al., 2020). Meanwhile, the effects for the Wards with the highest White populations are the opposite. The data in Figure 1 highlight how these disparities in the grocery gap fall across largely racial lines. | The misconception that city development does not need to be paired with affordable housing programs. People in these affected communities are viewed as dependents and don’t have a lot of power to make decisions to affect policies. |
Schools and food accessibility | Lack of sufficient nutritional education programs in schools to facilitate a nutrition-based rather than calorie-based approach to eating food. | The misconception that kids are wasteful and throw out food and don’t need to be involved in the process of deciding what is on a school lunch (Anacostia Community Museum) . |
2.2.3 Data on Income, Race, and Access to Full-Service Grocery Stores
Figure 1: The relationship between income, race, and access to full-service grocery stores (Jensen et al., 2020) | ||||||||
Ward | Full-Service grocery stores (2020) | Population (2020) | Median Household income ($) (2017) | % Individuals below the poverty line (2020) | % Black (2020) | Median Walk score | Median Transit Score | % Car Ownership (2020) |
1 | 10 | 91,498 | 93,284 | 13.6 | 21.7 | 79 | 88 | 54.5 |
2 | 11 | 92,509 | 104,504 | 13.3 | 13.6 | 89 | 92 | 53.5 |
3 (richest) | 16 | 84,869 | 122,680 | 8.1 | 5.4 | 54 | 60 | 77.6 |
4 | 11 | 86,660 | 82,625 | 11.2 | 47 | 66 | 58 | 76.1 |
5 | 9 | 90,479 | 63,552 | 15.9 | 56.6 | 63 | 58 | 70.0 |
6 | 14 | 103,316 | 102,214 | 12.1 | 39.7 | 78 | 91 | 67.3 |
7 (second poorest) | 2 | 80,951 | 40,021 | 26.6 | 92.0 | 63 | 48.5 | 58.1 |
8 (poorest) | 1 | 80,552 | 31,954 | 34.2 | 92.0 | 63 | 43 | 57.8 |
D.C. Overall | 74 | 710,834 | 90,695 | 16.8 | 44.5 | 71 | 69 | 64.1 |
3. Systems Thinking Approach
3.1 Systems Map

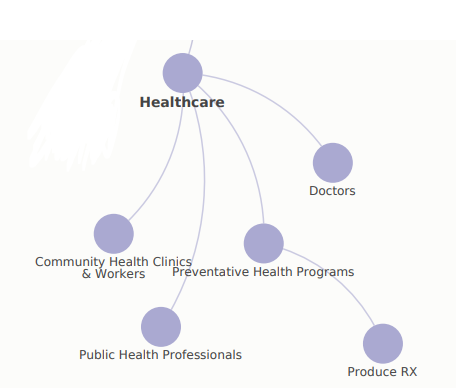
3.2 Stakeholders & Solutions Map
A wide range of stakeholders are involved with perpetuating root causes of food inaccessibility and initiatives working to improve the issue. These include community members, educational institutions, healthcare organizations, corporations, nonprofit organizations, and government officials who often collaborate to create many existing and former solutions in DC, including tax incentives for grocery stores and Produce RX. Looking at the actions of each existing stakeholder group helps effectively convey the range of existing solutions and reasons why they are insufficient.

4. Stakeholders and Solutions
4.1 Local Community

Local initiatives are uniquely rooted in the community and have great potential for sustainable change. Existing community-based solutions include mutual aid organizations which foster empowerment through community members donating when they can to collective food pantries like DC Fridge. Market 7 is an example of a community-oriented retail development that employs vendors from Wards 7 and 8 to create a food hall with culturally competent food for its residents. Co-ops and community gardens aim to empower community members to have agency over their own food by creating spaces for them to grow the healthy food they consume. However, resource scarcity can limit the extent of impact at times.
4.2 Educational Institutions

Educational institutions are home to many locally and federally funded nutrition reform programs in D.C. The importance of free and reduced lunches for adequate nutrition for many children leads organizations like D.C. Central Kitchen to focus on reforming the quality of lunch programs to ensure they are meeting children’s nutritional needs. D.C. Central Kitchen has specifically focused on centering kids as stakeholders in deciding what nutritious foods they want to reduce food waste and increase nutritional intake. Schools are inextricably linked to food security, as it is their responsibility to provide lunches and food programs for students in need. Additionally, they are often the sites of community initiatives around food. Over 50% of schools in Washington D.C. have urban farms (Reichler), and during the height of the pandemic, they were grocery distribution centers. Parents also have immense lobbying power to push for their children’s health by advocating for better programs. Utilizing schools as community catalysts to collectivize as agents for change can powerfully represent community members’ voices. However, issues still remain when it comes to effectively mobilizing community members and finding members who have the time to invest in advocacy when many have high work and family obligations.
4.3 Government

The D.C. City Council and federal government are responsible for addressing the needs of D.C.’s communities, especially the pressing disparities that impact Wards 7 and 8. Through policy and publicly funded initiatives, governments have the power to incentivize other actors including corporations, nonprofits, and healthcare professionals to take effective action around increasing food accessibility, and provide funding to schools for nutrition programs. However, many government programs fail due to a lack of community input that results in often misguided initiatives, bureaucratic issues, partisanship that slows down policy implementation, and lingering impacts of policies over the past century that intentionally marginalized Black and Brown communities. Moreover, welfare programs continue to be difficult to access due to limited locations and personnel, and stereotypes around users of welfare programs affect efforts to expand access. Recent government-sponsored initiatives to address food insecurity include a $56 million fund to incentivize grocery stores to open in Wards 7 and 8 (Jensen et al., 2020). This has been successful at attracting a Lidl to plan to open in Ward 8. However, these initiatives need to be paired with education surrounding nutrition and impacts of cash vouchers to maximize their effectiveness.
4.4 Nonprofits

Nonprofit organizations exist due to the existing community need for better food access. They operate across D.C. using a combination of grants from government sources like the Department of Health and Human Services and private donations to fund both donation-based and community-centered initiatives to increase food accessibility. Donation-based organizations include food banks like Capital Area Food Bank, which provides food donation boxes at schools, community centers, and at their facility in Northeast DC. DC Central Kitchen embodies a holistic community-centered approach by focusing on the systemic issues that perpetuate food insecurity like economic disparities, incarceration rate, and community empowerment by training former felons on probation to work in food-service jobs with the organization (Reichler). However, nonprofits still face challenges of communicating in culturally sensitive and effective ways with communities to inform them of available initiatives and resources, as well as garnering community input. One noteworthy model is DC Central Kitchen’s Champions Program, which involves two community members from Ward 8 as part of their organizing committee to provide insight into the community’s needs.
4.5 Corporations

The corporate food industry plays a large role in perpetuating the lack of access to stores and restaurants with healthy, affordable options for residents of Wards 7 and 8. Food corporations can choose to break the cycle of the lack of grocery stores and restaurants with healthy options by opening stores in Wards 7 and 8 to end the grocery gap, and employing local community members to foster economic prosperity within the region. However, without external incentives from government actors, they are unlikely to do this. Healthy Corners is a branch of the nonprofit DC Central Kitchen that works with convenience store owners to provide small quantities of fresh produce that can be bought in their stores to expand access to healthy food within existing establishments. Although this is important, it still does not address the grocery gap or give community members equitable access to healthy food compared to other parts of DC.
4.6 Healthcare Industry
Access to food and related systemic problems including cyclical poverty and educational equity impacting residents of Wards 7 and 8 are public health issues that healthcare professionals should address from a healthy equity perspective. Residents of Wards 7 and 8 face higher rates of heart disease, diabetes, and other health conditions preventable with adequate nutrition access and education (Baker, 2021). This contributes to a lower life expectancy for Black men and women in D.C. compared to other residents in the district. Medical and public health professionals can lobby for better nutrition education and the importance of access to healthy foods by recognizing these trends and advocating for measures to change them. Examples include the Produce RX program, which allows medical professionals to prescribe eating fresh fruit and vegetables to patients with diet-related chronic illnesses (Anacostia Community Museum). The prescription gives patients access to financial assistance to fund these purchases. Although this program has been especially effective, issues of transportation to grocery stores remain a barrier to residents’ ability to take advantage of this program (DC Greens).
4.7 Existing Global Solutions
4.7.1 World Food Programme (WFP)’s Fresh Food Voucher (FFV) Programme in Ethiopia’s Amhara Region
The success of Ethiopia’s FFV programme has been highlighted by the UN (Rooney, 2021). Given the millions of chronically food-insecure households in Ethiopia (United Nations, 2022), this program aims to combat malnutrition and food insecurity. Since 2017, WFP has provided 27,000 vulnerable households with monthly e-vouchers to purchase fresh food (Nutrition for Growth, 2021). The program specifically targets the ‘first 1,000 days’ for the extremely poor, including households with pregnant and lactating women and children under two years of age (Rooney, 2021). WFP also operates alongside a Social and Behavioral Change (SBCC) campaign, which offers school feeding programs and support to smallholder farmers. These additional educational components, aligned with Ministry of Health guidelines, simultaneously strengthen the resilience of the most economically vulnerable communities (Nutrition for Growth, 2021).
By addressing access through vouchers, utilization (SBCC), and availability (ag-production, processing, and supplying), this solution highlights the importance of cross-sector collaboration and tackling food insecurity holistically. The educational component enabled beneficiaries to effectively utilize their vouchers, allowing communities to improve their diet diversity over time—from 13-80% and 1-95% for children and mothers, respectively (Nutrition for Growth, 2021). This solution can also be replicated in other contexts, provided that access to mobile phones and network connectivity as well as an SBCC strategy developed through informative research (Nutrition for Growth, 2021).
4.7.2 Participatory Urban Agriculture Program (AGRUPAR) in Quito, Ecuador
AGRUPAR was launched by the Municipality of Quito in 2002 to improve food producers’ livelihoods, job creation, food and nutrition security, and democratization of the food system (foodpolicy.org, 2021). This program supports agricultural activity at every stage of the food chain—by “producing, processing, and distributing healthy food from urban and peri-urban gardens” (FAO, 2018). It has successfully advanced food security and socioeconomic outcomes, particularly for vulnerable groups such as women, the elderly, and people with disabilities (FAO, 2018).
This solution has been recognized for its participatory and holistic approach which incorporates the most vulnerable groups (FAO, 2018). Through its four main axes—community training to encourage urban and home gardening, support for market-oriented local production through microenterprise formation, organic produce markets and farmer networks to promote food supply and distribution, and educational bio-fairs to promote healthy diets and nutrition—it demonstrates the importance of an integrated approach (FAO, 2018). AGRUPAR recognizes how urban agriculture and food security may cooperate with the broader principles of sustainability and equity to benefit the entire community. This program can serve as a model for food policy that centers a food system approach in other communities.
4.7.3 La Via Campesina
La Via Campesina, founded in 1993 in Mons, Belgium, represents an international peasant movement fighting for food sovereignty as an alternative model to industrial food production. With members from 182 organizations in 81 countries (Wikimedia, 2022), this movement centers on questions of power and control to change how people think about food, their relationship with food, and their relationship with other people (Provost, 2013). They operate under the belief that food security is best achieved when food production is centered among the hands of the hungry or produced locally (Wikimedia, 2022), and they focus on training, education and communication, and exchanging generations of accumulated knowledge (Provost, 2013) to ensure that healthy, nutritious, affordable, culturally appropriate, and locally produced food is a human right for all (Wikimedia, 2022).
4.8 Insights and Takeaways: Stakeholders and Solutions
An analysis of the different stakeholders involved in perpetuating food accessibility issues and solutions surrounding them highlight a few key takeaways important to keep in mind when understanding why existing initiatives in DC fail. Siloing initiatives instead of collaborating more across stakeholders limits efficacy and impact. Additionally, insufficient community input leads to initiatives not properly curated to community needs.
5. Recommendations, Key Insights, and Lessons Learned
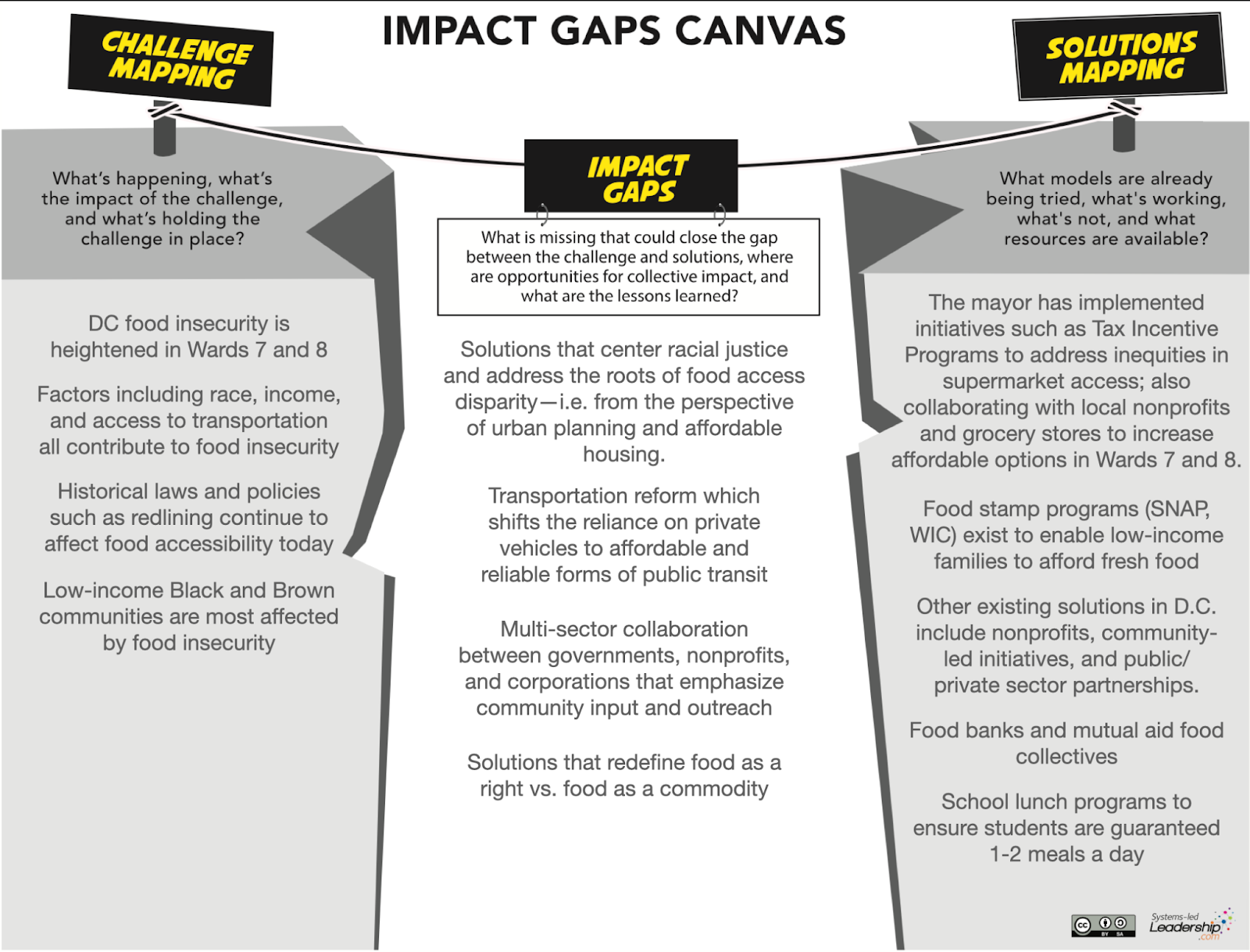
5.1 Impact Gap Canvas
5.2 Centering the Agency, Identity, and Humanity of Communities

One of the most important takeaways from our research is the importance of meaningful community input. For example, D.C. Central Kitchen’s Champions Program is the key component to their organization’s effectiveness and success in reaching the community. Not only is this relationship important in terms of outreach and ensuring that these services reach the targeted beneficiaries, but it also tackles the misconception and mental model that improving food access must be a charitable relationship. Like mutual aid, it promotes shared solutions and ensures that all voices are included in decision-making to benefit everyone in the community. Shift from nominal/instrumental participation to representative/transformative participation that amplifies their voices and promotes lasting change (Han et al., 2019).
5.3 Cross-Sector Collaboration

Engaging different stakeholders is important to provide a comprehensive overview of the solutions landscape. Solutions may already exist within communities, but they must be realized and scaled by budgetary investments to support the expansion of programs, and this level of scaling will require cross-sector partnerships and public/private collaborations. Any initiative to increase food security must also be paired with nutritional education to ensure a quality diet (Han et al., 2019).
5.4 Invest in Public Transportation Infrastructure

In June 2019, Mayor Bowser launched a pilot program, Taxi-to-Rail (T2R), to address the lack of transportation access in Wards 7 and 8. This initiative provided rides to essential amenities such as Metro Rail stations, grocery stores, pharmacies, etc. Residents who used T2R were reimbursed up to $15. While this program was officially discontinued during the pandemic, its initial launch was unsuccessful: not only was this service inaccessible for individuals who didn’t have a phone to call a taxi, but the cost of taxi rides often exceeded the $15 reimbursement fee, leaving riders stranded mid-trip (Jensen et al., 2020). This example, paired with the data indicating that low access to public transit is highly correlated with food insecurity in Wards 7 and 8, emphasizes the need to invest in public transportation infrastructure. Additionally, this investment must address the frequency and reliability of public transportation to ensure that residents are provided with safe and convenient experiences to access the food they need.
5.5 Center Racial Equity

Issues of food security in Wards 7 and 8 are rooted in systemic racism and intentional efforts by the government and white community members to exclude Black and Brown communities and maintain historical social and economic hierarchies. Without recognizing the significant impact that policies like redlining continue to have on communities today, solutions that address systemic roots will not emerge. Therefore, centering racial equity is key to any successful initiative. This has proven to be true with organizations like D.C. Central Kitchen’s model of recognizing the intersectionality between incarceration rates for Black and Brown Americans, job security, racism, and food access to affect community-centered, sustainable change.
5.6 Food as a Right
Focusing on food justice, not just food accessibility is important to work towards sustainable solutions that aim to secure the right to healthy food for all residents of DC rather than bandaid the disparities faced by Wards 7 and 8 residents. Shifting away from profit-centered motivations that view food as a commodity and centering securing the right for food is the approach that many local community-based organizations have taken and is key to sustainable change.
5.7 Final Reflections
Our recommendations focus on the fundamental values of centering community and racial equity that are important to the success of any solution, and addressing the structural issue of transportation access to make healthy food more accessible. Although these do not address or guide all stakeholders and systems, this grounds a starting point that moves towards effective systemic action.
A significant obstacle to implementing existing initiatives and our recommendations is the challenge of communicating with communities in Wards 7 and 8 in a sensitive and culturally competent way (DC Central Kitchen). Although this may pose challenges to our recommendations, it emphasizes the importance of centering community and racial equity.
Although our research attempts to represent the systemic roots and intersectionality between the many social issues impacting residents of Wards 7 and 8, we recognize that there is still more to explore to understand the extent of the impacts on residents, challenges to solutions, and organizations that should be uplifted for the effective work they are doing. However, we believe that a significant outcome of our research is the strength of the interconnections between the different social structures explored and the need to recognize and take advantage of those interconnections to foster collaboration. We hope that this report provided a comprehensive overview, and look forward to further exploring the issue.
7. Appendix
7.1 Definitions
Term | Definition (Jensen et al., 2020) |
D.C. Wards | The District of Columbia is divided into eight wards, each with approximately 75,000 residents, and each represented by an elected member of the D.C. Council and local bodies of government called Advisory Neighborhood Commissions. |
Food Access | Accessibility to sources of healthy food, as measured by distance to a store or by the number of stores in an area. Individual-level resources, such as family income or vehicle availability, and neighborhood-level indicators of resources, such as the average income of the neighborhood and the availability of public transportation, may affect accessibility. |
Food Apartheid | This refers to the policies and systems that result in disproportionate access to food by different geographical areas, communities, races, and socioeconomic statuses, resulting in food deserts and food swamps. |
Food Desert | Geographical area with limited access to affordable and nutritious food, particularly an area composed of predominantly lower-income neighborhoods and communities; a significant number (at least 500 people) or share (at least 33 percent) of the population is greater than 1.0 mile from the nearest supermarket, supercenter, or large grocery store for an urban area or greater than 10 miles for a rural area. |
Food Insecurity | The condition is assessed in the food security survey and represented in food security reports from the U.S. Department of Agriculture. It is a household-level economic and social condition of limited or uncertain availability of nutritionally adequate and safe foods or limited or uncertain ability to acquire acceptable foods in socially acceptable ways. |
Food Sovereignty | A food model which centers the needs and ability of communities to secure access to healthy and culturally competent food as opposed to focusing on market demands (U.S. Food Sovereignty Alliance, 2021). |
Full-service grocery store | Business establishments with a minimum of 50% of the store’s total square footage, or 6,000 square feet, primarily engaged in retailing designated food products for home consumption and preparation. |
7.2 Research questions
- How do historically racist policies create disparities in food access and security?
- How does historical urban planning affect food accessibility in marginalized communities in D.C. today?
- How has gentrification affected or exacerbated issues of food security?
- Think about the rising cost of living and how that affects the efficacy of current solutions to food insecurity in the region
- How do current initiatives from the mayor’s office affect issues of food security for marginalized communities?
- What are some existing non-profit initiatives that aim to combat issues of food injustice in D.C.?
7.3 Interview questions
- Why is your work needed in the context of food insecurity?
- Why have existing solutions failed, and what does your organization do differently?
- Who are the people you serve? What are the stories they are telling you?
- How do people get help from you? How do you outreach to communities in need to inform them about the work that you do?
- What would you do differently if you had unlimited resources?
- What do people and/or government get wrong about food poverty?
- How have/do urban planning policies and gentrification shape food insecurity and access in DC, particularly in Wards 7 and 8?
- How do you view the roles of different stakeholders including nonprofit organizations and government initiatives in combatting food insecurity?
- What do you believe is the main driver of the racial inequalities/dynamics that define who are most affected by food insecurity here?
- What other actors do you think we should talk to?
- Is there anything we should keep in mind or know as we’re working to understand systemic food insecurity in DC?
- How has COVID impacted food accessibility/security and the work that you do?
- Are there any global or national initiatives that your organization draws inspiration from? What are similar models that you are aware of happening around the country and/or the world?
- What are some misconceptions/myths that you have realized about this space since working with this organization?
- What have been some of the greatest challenges to your work and how have/are you working to overcome them?