
Today’s Date: ________________________
Name______________________________________________ Date of Birth:_______________
Social Security Number: _______-______-_______
Address: ______________________________________________________________________________
______________________________________________________________________________________
Phone Number: ___________________________ Email: ______________________________________
Would you like to be reminded of appointments? Yes No. If yes, prefer email, phone call or text?
Insurance, Primary:_________________________________ Member Number: ____________________
Insurance, Secondary (if applicable):_____________________ Member Number: ___________________
Responsible Party: Self______ Other (please specify): _________________________________
Name of Emergency Contact:_______________________________________________________________
Phone Number of Emergency Contact:________________________________________________________
Please check the appropriate box for YOUR medical history
High blood pressure___ Diabetes___ Arthritis___ COPD/Asthma___ Smoker___ Cancer___
Heart Problems___ Pacemaker___ Other (please specify):________________________________________
Surgical History: _______________________________________________________________________________
If female, are you currently pregnant? Yes No
Primary Physician: __________________________ Referring physician:______________________________
Do you have any medication allergies? Yes No If so, what? ____________________________________
Please list your current medications, including any over the counter medications. List name, dosage and how often taken. OR please attach a list of your current medications.
________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Name: _____________________________________________________________ Date: ____________
Date of onset of injury or illness:___________________________________
Height: _____________ Weight: ____________ BP: _____________ Pulse: _____________
Did you have surgery? Yes No If, so, what surgery?________________ Date:__________________
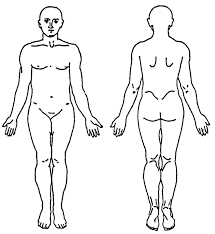
What is your chief complaint? _______________________________________________________________ ________________________________________________________________________________________
Have you ever had a previous injury or occurrence to this area? Yes______________________ No
Have you been treated for this in the past? Yes__________________________________ No
Are you having any difficult: Balancing? Yes No Walking? Yes No Lifting? Yes No
Scale of 0 to 10 (0 is no pain and 10 is the worst pain imaginable), circle the appropriate number.
Current level of pain: 1 2 3 4 5 6 7 8 9 10
Least amount of pain over the last week: 1 2 3 4 5 6 7 8 9 10
Highest level of pain over the last week: 1 2 3 4 5 6 7 8 9 10
What increases your pain? _______________________________________
What decreases your pain?_______________________________________

Cancellation/Attendance/Late Policy
We take pride in providing quality rehabilitation service to our patients. In order to receive maximum benefit from your therapy treatments, we ask a few things of our patients;
- We ask that you arrive on time for your therapy appointments. If you arrive 15 minutes late, we reserve the right to reschedule your appointment.
- If you are unable to keep your appointment, we ask that you notify us by 10:00am the day prior to your appointment at 803-207-8177
- If we do not receive this advance notice from you, you will be charged a $30.00 cancellation fee prior to receiving your next scheduled treatment.
- In the event of three (3) appointments that have been missed with or without notification, we reserve the right to discharge you from your rehabilitation services.
- We ask that you perform your HEP (Home Exercise Program) as prescribed.
We look forward to working with you and helping you receive the best results from your therapy treatment. We thank you for giving us this opportunity.
Patient Signature: _____________________________________ Date: ________________
Insurance Verification
We will gladly file your insurance claim for you; however, LTC Therapy Solutions does not guarantee payment by the insurance company for services rendered. In the case that your claim or a portion there of is denied, you will be responsible for payment of the remaining balance.
Medicare Beneficiaries:
We are required, by law to inform you that Medicare Part B will cover 80% of the cost of therapy. The remaining balance may be covered by supplemental insurance coverage or may be paid out-of-pocket. After the claim is initially filed, you will receive a letter of denial from Medicare. We will receive the same letter of denial, and at that time LTC Therapy Solutions will bill the remaining claim with the supplemental insurance, if applicable.
Please direct any therapy concerns to Dr. Ashley Fann at 803.207.8177 or afann@agapesenior.com
Please direct any billing concerns to Iesha Wade at 803.207.8177 or iwade@agapesenior.com
I give permission for rehabilitative services to be performed by LTC Therapy Solutions, Inc. I will be responsible for payment for services, if the insurance company does not pay.
Patient Signature: ____________________________________ Date: ___________
Consent to Therapy Treatment
I hereby consent to the treatment of my condition by a licensed therapist. I understand that I have received an initial evaluation which will now be followed by one or several treatment sessions. These sessions may include one or more of the following: Joint mobilization or manipulation; soft tissue work; manual therapy; electrical stimulation; ultrasound; Heat/ice; mechanical and manual traction; passive/active range of motion; strengthening; stretching; exercise; and/or activity of daily living modification.
Patient or Guardian Signature: __________________________________Date:___________
Assignment of Benefits and Insurance Proceeds
I hereby authorize payment from my insurance company of medical benefits for services provided in Out Patient Therapy by an assignment of benefits. The completion of insurance forms and the assignment of insurance benefits do not relieve the undersigned of the obligation to pay the amount owed for Therapy.
Patient or Guardian Signature: __________________________________Date:___________
Who Will Be Responsible For This Bill?
Signature of Responsible Party:_________________________________________________
Date Responsible Party was notified:_____________________________________________
Signature of person who notified responsible party:__________________________________
Release of Information
I hereby authorize release of information necessary to file claims with my insurance company and information to my physician/s. I permit a copy of this authorization to be used in place of the original.
Patient or Guardian Signature: __________________________________Date:___________
Receipt of Privacy Practice
I have received a copy of The Notice of Privacy Practices and have had an opportunity to ask questions.
Patient or Guardian Signature:___________________________________Date:___________
Verbal Consent to:
Treat, Bill Insurance, Accept Responsibility of Charges Not Covered by Insurance, and Release of Information given to: __________________________________________________________
By POA Name: _______________________________Time:____________Date:_______