Opioid Working Group | headsUPmigraine |
Easy copy-paste-send advocacy! This report calls for an end to prescription opioid restrictions, which have greatly harmed people in pain without helping to reduce overdoses. Copy it, paste it in an email, and send it to your state lawmakers. Link to them below. If you’re a pain patient, add a few sentences to the first paragraph, explaining how you’ve been harmed by these restrictions. If you’d like to write a more personal letter, feel free to use this research as you see fit. If you’d like, you can say this report was written by Jill Piggott, PhD, Director of headsUPmigraine. But you are welcome to it without identifying its source. Please ask your family and friends to join us. If they’re not pain patients themselves, they can copy-paste-send this version of the letter. This letter is specific to state legislation. Link to legislators here: Thank you for joining our advocacy. Jill Piggott, PhD, Founding Director Nita Ghei, PhD, JD, Research Director ____________________________________________________________________ |
Dear [State Representative or Senator]: I’m a chronic pain patient, and I’ve been harmed by restricted access to FDA-approved medicine. Washington State lawmakers have introduced a bill that would help people like me, who are suffering with untreated pain, avoidable disability, and disease progression because our doctors know they might face serious consequences if they prescribe specific FDA-approved medicines. I hope you’ll consider introducing a similar bill here. Proposed state legislation to protect patient access to medicine: “The legislature finds that Washington residents suffering from chronic pain are unable to obtain necessary prescription medications at effective doses to treat their pain because previous opioid-related laws and rules have created a chilling effect among health care practitioners. These health care practitioners are afraid of facing discipline, losing their license to practice, and of possible civil liability if they prescribe high doses of opioids to patients with chronic pain. Therefore, the legislature intends to end the chilling effect created by these laws to allow patients in Washington with chronic pain to receive prescription medications at levels that effectively treat their pain.” The bill would add new sections to chapter 18.22 RCW to read as follows: “No [clinician] licensed under this chapter acting in good faith may be subject to civil liability or disciplinary action by the board or department for prescribing opioid drugs in excess or in violation of department and board rules to a patient with chronic pain who has requested such a prescription and has provided written informed consent.” Named clinicians are physicians and surgeons, dentists, physician’s assistants, and nurse practitioners. The CDC, FDA, and HHS have all warned doctors and policymakers about serious harms suffered by pain patients resulting from “misapplication of the 2016 CDC Guideline.” In 2019, three federal agencies identified serious harms people in pain are suffering in the wake of severe restrictions to the most effective FDA-approved medicines for the treatment of severe pain, including unnecessary disability and disease progression. Pain increases patient mortality from a range of diseases, including cancer, and is a risk for suicide even in patients without underlying depression. In 2019, the FDA issued new labeling for all opioids, warning doctors that discontinuation or rapid decreases in dose result in “serious withdrawal symptoms, uncontrolled pain, psychological distress, and suicide.” The FDA cautioned that “these symptoms can lead patients to seek other sources of opioid pain medicines, which may be confused with drug-seeking for abuse. Patients may attempt to treat their pain or their withdrawal symptoms with illicit opioids, such as heroin, and other substances.” Both the US Department of Health and Human Services and the Centers for Disease Control reiterated that the “CDC Guideline for the Prescribing of Opioids for Chronic Pain does not recommend opioid discontinuation when benefits of opioids outweigh risks.” HHS urged clinicians and policymakers like you to:
I think you’ll be more likely to support patient access to all FDA-approved medicines when you learn that large studies repeatedly show that patients rarely misuse or become addicted to prescription opioids.
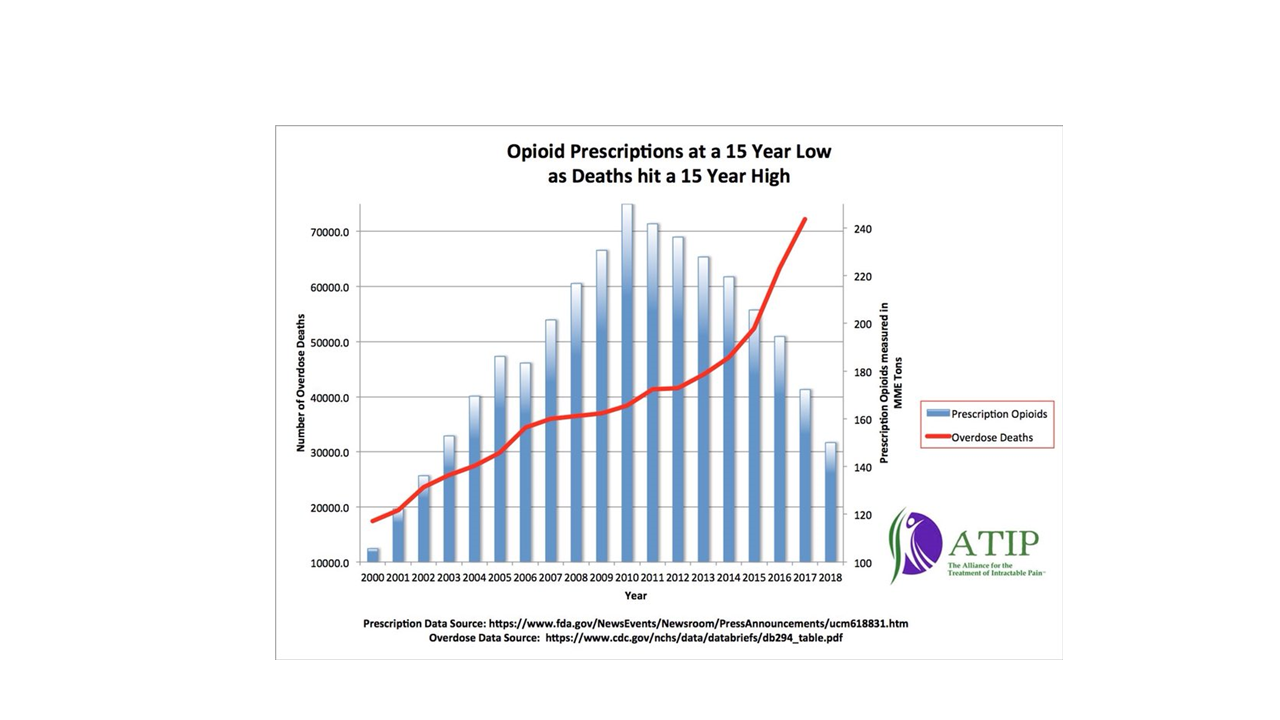
Restricting prescription opioids has failed to reduce overdose deaths. State overdose stats identify any drug that’s available by prescription as a “prescription opioid,” regardless of how the person obtained the drug. When researchers compare overdose deaths with prescription drug monitoring program data, they find only a small percentage had a prescription for a drug that killed them. Of the 2,916 people who died by opioid overdose in Massachusetts between 2013-2015, for example, only 39 (1.3%) had an active prescription for the opioids detected in their toxicology reports on the date of death (Walley 2019). Nor does data support the hypothesis that increased prescribing resulted in increased addiction. Again in 2019 as in years past, the National Survey on Drug Use and Health showed that the “dramatic increase in deaths involving prescription analgesics since 2000 cannot be explained by a dramatic increase in misuse or addiction rates, because there was no such increase.” The long-term upward trend in overdose deaths began in 1979 and appears to be a “problem of increasingly reckless polydrug use, a problem that cannot be solved—and may be worsened—by demanding wholesale reductions in pain pill prescriptions” (Sullum 2019). Research shows that efforts to curb opioid overdoses by restricting access to prescription medicines “have failed to demonstrate a consistent benefit on fatal or nonfatal opioid overdoses.” Complex mathematical modeling shows prescription drug monitoring programs, opioid prescribing guidelines, and dose-limit laws will have a “modest effect, at best, on the number of opioid overdose deaths in the near future,” which are expected to continue to rise. Evidence-based recommendations include “improving access to treatment, expanding harm-reduction interventions, and lowering exposure to illicit opioids, to curb the trajectory of the opioid overdose epidemic in the United States” (Chen 2019). Though well intended, current policies aimed at lowering OD rates by restricting patient access to medicine are failing people with addiction and directly harming people in pain, like me. I urge you as strongly as I can to introduce a bill like Washington State’s that protects patient access to FDA-approved medicine. Thank you. Sources: Brat GA, et al. “Postsurgical Prescriptions for Opioid Naive Patients and Association with Overdose and Misuse: Retrospective Cohort Study. BMJ. 2018 Jan 17;360:j5790. https://www.bmj.com/content/bmj/360/bmj.j5790.full.pdf Chen, Q., et al. “Prevention of Prescription Opioid Misuse and Projected Overdose Deaths in the United States.” JAMA network open. 2019 Feb 1;2(2). https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2723405 Ciesielski T, Iyengar R, Bothra A, Tomala D, Cislo G, Gage BF. “A Tool to Assess Risk of de Novo Opioid Abuse or Dependence.” American Journal of Medicine. 2016 Jul 1;129(7):699-705. https://www.amjmed.com/article/S0002-9343(16)30202-9/fulltext Food and Drug Administration (US). “FDA identifies harm reported from sudden discontinuation of opioid pain medicines and requires label changes to guide prescribers on gradual, individualized tapering.” 2019. Health and Human Services (US). 2019. HHS Guide for Clinicians on the Appropriate Dosage Reduction or Discontinuation of Long-Term Opioid Analgesics. https://www.hhs.gov/opioids/sites/default/files/2019-10/Dosage_Reduction_Discontinuation.pdf Sullum, Jacob. “New Survey Data Confirm That Opioid Deaths Do Not Correlate With Pain Pill Abuse or Addiction Rates.” Reason 21 Aug 2019. https://reason.com/2019/08/21/new-survey-data-confirm-that-opioid-deaths-do-not-correlate-with-pain-pill-abuse-or-addiction-rates/ Walley AY, et al. “The contribution of prescribed and illicit opioids to fatal overdoses in Massachusetts, 2013-2015.” Public Health Reports. 2019 Nov;134(6):667-74. https://journals.sagepub.com/doi/abs/10.1177/0033354919878429?journalCode=phrg Washington State. H-4050.1: House Bill 2807, 66th Legislature (2020). http://lawfilesext.leg.wa.gov/biennium/2019-20/Pdf/Bills/House%20Bills/2807.pdf?q=20200123195615
|
Source: The Alliance for Treatment of Intractable Pain (ATIP) |