
Research
The cost of type 1 diabetes: a nationwide multicentre study in Brazil Roberta Arnoldi Cobas,a Marcos Bosi Ferraz,b Alessandra Saldanha de Mattos Matheus,a Lucianne Righeti Monteiro Tannus,a Carlos Antonio Negrato,c Luiz Antonio de Araujo,d Sergio Atala Dibb & Marilia Brito Gomesa for the Brazilian Type 1 Diabetes Study Group
Objective To determine the direct medical costs of type 1 diabetes mellitus (T1DM) to the National Brazilian Health-Care System (NBHCS) and quantify the contribution of each individual component to the total cost. Methods A retrospective, cross-sectional, nationwide multicentre study was conducted between 2008 and 2010 in 28 public clinics in 20 Brazilian cities. The study included 3180 patients with T1DM (mean age 22 years ± 11.8) who were surveyed while receiving health care from the NBHCS. The mean duration of their diabetes was 10.3 years (± 8.0). The costs of tests and medical procedures, insulin pumps, and supplies for administration, and supplies for self-monitoring of blood glucose (SMBG) were obtained from national and local health system sources for 2010–2011. Annual direct medical costs were derived by adding the costs of medications, supplies, tests, medical consultations, procedures and hospitalizations over the year preceding the interview. Findings The average annual direct medical cost per capita was 1319.15 United States dollars (US$). Treatment-related expenditure – US$ 1216.33 per patient per year – represented 92.20% of total direct medical costs. Insulin administration supplies and SMBG (US$ 696.78 per patient per year) accounted for 52.82% of these total costs. Together, medical procedures and haemodialysis accounted for 5.73% (US$ 75.64 per patient per year) of direct medical costs. Consultations accounted for 1.94% of direct medical costs (US$ 25.62 per patient per year). Conclusion Health technologies accounted for most direct medical costs of T1DM. These data can serve to reassess the distribution of resources for managing T1DM in Brazil’s public health-care system.
Introduction
tion rate and inpatient costs among people with diabetes were
Type 1 diabetes mellitus (T1DM) is a chronic lifelong disease, commonly diagnosed in youth, that requires strict multidis- ciplinary treatment for the patient’s entire life.1 Over the last decades, the incidence of T1DM has been increasing in most regions of the world.2,3 In the State of São Paulo in Brazil, the average annual incidence of T1DM between 1987 and 1991was 7.6 per 100 000.4 Additionally, in the city of Bauru in the same state, the incidence of T1DM in children younger than 15 years, increased 9.6 times from 1986–2006, especially among children of low socioeconomic status between the ages of 5 and 9 years.5
T1DM is associated with long-term complications that cause high morbidity and mortality,6 affect the quality of life and increase health-care costs.7,8 In the Diabetes Control and Complications Trial (conducted from 1983 to 1993) and its follow-up study, known as the Epidemiology of Diabetes In- terventions and Complications study (DCCT/EDIC), which
434
2.1- and 2.2-fold greater, respectively, than among the general population.12 Most costing studies on diabetes include both T1DM and type 2 diabetes mellitus (T2DM),8 or only T2DM.13 Hence, little is known about the impact of T1DM alone.12 Although previous studies have investigated the costs associ- ated with diabetes in Brazil,7,14 the impact of T1DM alone has never been assessed.
The objective of this study was to perform a partial eco- nomic evaluation of the direct medical costs of T1DM, from the public health-care system’s perspective, in a representative sample of patients attending the public health-care system in Brazil. We also aimed to identify and quantify the contribu- tion of individual determinants to the total direct costs. Data on the use of resources and on the costs of T1DM from the public health-care system’s perspective will allow health-care providers to better understand the effects of the disease, define management strategies and appropriately allocate resources.
assesses incidence, predictors of complications, and the impact and cost-effectiveness of intensive versus standard control,
Methods intensive control has been shown to reduce the development of microvascular and cardiovascular complications2,9 and to
Study design
be cost-effective.10 Nonetheless, approximately one third of the
This study was a retrospective, cross-sectional cost-of-illness patients who participated in our study were not screened for
study conducted nationwide at multiple centres between chronic complications over the previous year and the majority
December 2008 and December 2010. The centres were 28 did not meet metabolic control goals.11
Brazilian secondary and tertiary public care clinics located In the United States of America, average health expendi-
in urban centres in four geographic regions of Brazil: north/ ture is 2.3-fold higher for people with diabetes than for people
north-east, mid-west, south-east and south. All patients re- without the disease.8 In a study in Scotland, the hospitaliza-
ceived health care from the National Brazilian Health Care
a State University Hospital of Rio de Janeiro, Boulevard Vinte oito de Setembro, 77-Vila Isabel, 20551030, Rio de Janeiro, Brazil. b Federal University of São Paulo, São Paulo, Brazil. c Bauru Diabetics Association, Bauru, Brazil. d Joinville Endocrinology and Diabetes Institute, Joinville, Brazil. Correspondence to Roberta Arnoldi Cobas (e-mail: robertacobas@gmail.com). (Submitted: 24 July 2012 – Revised version received: 10 February 2013 – Accepted: 18 February 2013 – Published online: 4 April 2013 )
Bull World Health Organ 2013;91:434–440
|
doi: http://dx.doi.org/10.2471/BLT.12.110387

Bull World Health Organ 2013;91:434–440
Research Roberta Arnoldi Cobas et al. The cost of type 1 diabetes in Brazil System (NBHCS). We determined the number of patients enrolled in the study in each region on the basis of the estimated prevalence of T1DM in Bra- zil and the population density in each geographic region. Since patients with T1DM in Brazil are usually treated at secondary or tertiary centres, primary care centres were not included in the study. Each clinic provided data from at least 50 consecutive outpatients with an initial diagnosis of T1DM who regularly attended the clinic. Data were collected through interviews during clinic visits using a chart form. The detailed meth- ods have been described elsewhere.11 Written informed consent for the study was obtained from all patients aged 18 years or older or from the parents or guardians of patients younger than 18 years. The study was approved by each local centre’s ethics committee. Only patients who had had at least 12 months of follow-up at the centre were included in the cost-of-illness study. This inclu- sion criterion allowed us to quantify the variables required to determine costs over the year that preceded the study. Clinical and demographic variables
We obtained demographic data and data on economic status and defined economic status according to the Brazil- ian Economic Classification Criteria,15 used to estimate the purchasing power of urban individuals and families and to classify the urban population into economic strata. These criteria provide scores based on the ownership of items and educational level.15 We defined the duration of the diabetes as the time elapsed since the diagnosis.
During the clinic interviews we obtained information on diabetic treatment modalities; source of insu- lin pumps, medications and supplies for self-monitoring of blood glucose (SMBG); frequency of SMBG, and routine diabetes care. We obtained the following information from medi- cal records: total number of glycated haemoglobin (HbA1c) measurements over the prior year, fructosamine levels, fasting and 2-hour postprandial gly- caemia, total cholesterol, low-density lipoprotein (LDL), high-density lipo- protein (HDL), triglycerides, uric acid, plasma creatinine, plasma urea, sodium, potassium, liver enzymes (aspartate [AST] and alanine aminotransferase [ALT]), C-reactive protein (CRP),
thyroid-stimulating hormone (TSH), urine protein and urine albumin. We recorded the number of tests performed to screen for complications of diabetes, such as electrocardiograms, exercise stress tests, stress echocardiographs, calcium score tomographies, coronary artery angiographs and fundoscopies. We also analysed the frequency of vari- ous medical procedures, such as vitrec- tomy, laser therapy and haemodialysis, and of hospitalizations due to diabetes decompensation or ketoacidosis. Costs and health-care resource distribution
We calculated direct medical costs from the costs of medications (oral drugs and insulin), SMBG supplies, blood analysis and other tests, consultations with physicians, nurses and dietitians, medical procedures and hospitaliza- tions during the preceding year. The drugs included in the analysis were those used specifically to treat T1DM or its comorbidities (arterial hyperten- sion, dyslipidaemia, obesity) and related complications (diabetic nephropathy/ chronic renal failure, neuropathy and neuropathic pain, retinopathy, cardio- vascular disease). We also included the costs of the nutritional supplements given to patients with chronic renal failure or neuropathy, such as calcium, vitamin D and vitamin B12. In the case of drugs provided by public institutions, we obtained the costs from the web site of the Brazilian Ministry of Health16; for drugs that were privately acquired, we used the average price found in three nationwide pharmaceutical web sites. These privately-acquired drugs include medications or supplies that are not standardized by the health system. When the price varied by region, we calculated an average cost. We obtained the costs of tests and medical procedures from a 2010–2011 NBHCS source that gives the prices used to reimburse public health-care units. The cost of insulin pumps and administration supplies was based on what the Municipal Health Bureau of Rio de Janeiro (RJ-SMS) paid in May 2010 (Roche®). We determined the costs of SMBG supplies from what the RJ-SMS paid in April 2011 or, when privately acquired, by calculating the mean costs for three nationwide phar- maceutical companies.
We converted all costs to United States dollars (US$) using a conversion rate of US$ 1.00 = 1.9315 reais, which
was the average for the period from 2008 to 2010. Data storage and statistical analysis
We used Excel 2010 for Windows to store the data and we performed the statistical analysis with SPSS ver- sion 17.0 (SPSS Inc., Chicago, United States of America). The data are pre- sented in Table 1 as count (percentage), mean ± standard deviation (SD) and me- dian followed by its interquartile range. The costs are presented as means with their 95% confidence intervals (CIs). We log-transformed the non-normally distributed variables and compared means using t-tests or ANOVA.
Results
Of the 3591 patients initially evaluated, 3180 were included in this study. The study population consisted of 56.3% females and 57.4% Caucasians. The av- erage age was 22 years (SD: ± 11.8) and average disease duration was 10.3 years (SD: ± 8.0). Table 1 shows the demo- graphic and economic data pertaining to the study population.
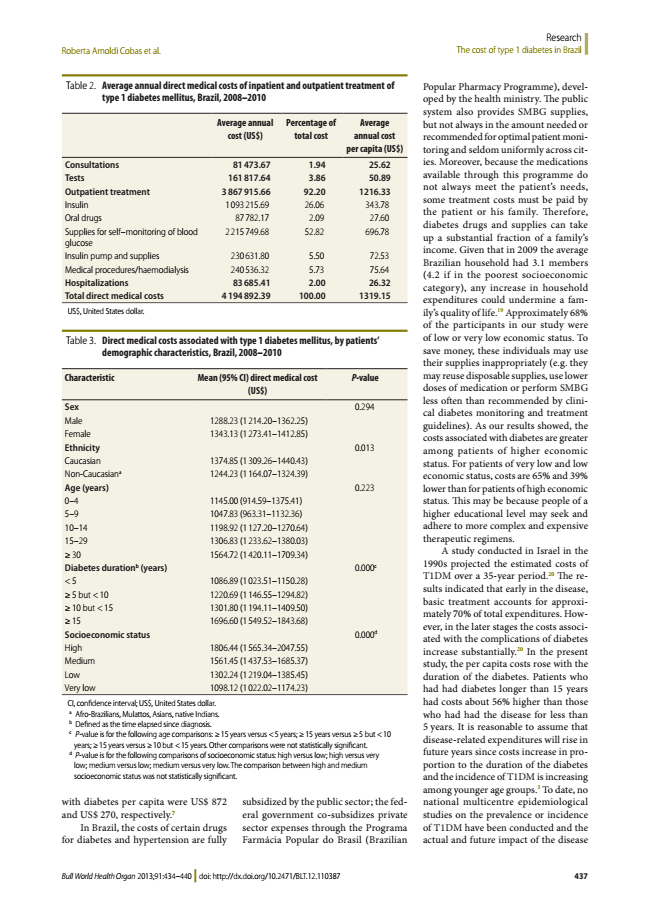
The overall direct medical cost per capita was US$ 1319.15. The expenditure related to treatment – US$ 1216.33 per patient per year – represented 92.20% of this total direct medical cost. Insulin ad- ministration supplies and SMBG – US$ 696.78 per patient per year – accounted for 52.82% of total direct medical costs. The expenditure on insulin pump and its supplies represented 5.5% of the to- tal direct cost. Only 38 (1.2%) patients used this treatment modality, at an average cost per patient of US$ 6069.26. Medical procedures and haemodialysis accounted for 5.73% – US$ 75.64 per patient per year – of the direct medical costs. The cost of consultations – US$ 25.62 per patient per year – accounted for 1.94% of direct medical costs. The data are presented in Table 2.
The direct medical costs associated with T1DM, stratified by patients’ de- mographic characteristics, are presented in Table 3. We found no significant dif- ferences in costs by sex and age range. However, the longer the duration of the diabetes and the higher the socioeco- nomic status, the higher the costs. Costs showed a significant 1.56-fold increase between diabetes of less than 5 years’ duration and diabetes whose duration was 15 years or longer. Similarly, costs
|
doi: http://dx.doi.org/10.2471/BLT.12.110387 435

Research The cost of type 1 diabetes in Brazil Roberta Arnoldi Cobas et al.
Table 1. Clinical and demographic characteristics of patients with type 1 diabetes
mellitus (n = 3180), Brazil, 2008–2010
were a significant 1.65 times higher among patients in the high socioeco- nomic stratum than among patients in the socioeconomic stratum classified as very low.
Discussion
This study is the first to estimate the di- rect medical costs of T1DM in a Brazil- ian sample of patients. T1DM represents an average cost of US$ 1319.15 per pa- tient for the NBHCS. Importantly, most expenditures were related to therapy, largely insulin, and to SMBG supplies, which are items that all patients with T1DM require. These requirements may explain why the per capita medical
respectively), followed by prescription drugs other than insulin (39 and 26%, respectively) and inpatient expenditures
Characteristic Female sex, no. (%) Mean age, years (SD) Value
1791 (56.3) 22 (11.8)
(18 and 17%, respectively).17 These find- ings are consistent with ours because medications and blood glucose monitor- ing accounted for the largest fraction of Age range, years (%)
the direct costs in our study. 0–4 51 (1.6)
As shown, treatment technologies 5–9 308 (9.7)
accounted for most public expendi- 10–14 604 (19)
ture; human resources accounted for 15–29 1471 (46.3)
little expenditure. These differences in ≥ 30 746 (23.5)
the apportionment of Brazilian public Ethnicity, no. (%) Caucasian Non-Caucasiana Socioeconomic status,b no. (%) High Medium Low Very low Occupation, no. (%) Current worker health resources must be carefully
1824 (57.4) 1356 (42.6)
examined because more money is be- ing spent on SMBG supplies than on physician and dietitian consultations
222 (7.2) 710 (22.3) 1052 (33.1) 1102 (34.7)
and nurse counselling. These findings point to the need to pay greater, more logistical and financial attention to the integral health assistance model, which involves investing in a multidisciplinary
997 (31.4)
team and focusing on health education and on the rational and effective use of Unemployed 232 (7.3)
the procedures and technologies avail- Temporarily medically disabled by NISS 52 (1.6)
able. The complex treatment of T1DM, Retired because of diabetes 85 (2.7)
which requires vigilance and frequent Student 1483 (46.6)
monitoring, underscores the importance Otherc 331 (10.4)
of the physician–patient relationship in Level of care, no. (%)
establishing a partnership conducive Secondary Tertiary Mean diabetes duration,d years (SD) HbA1c, % (SD) With microvascular complications,e no. (%) With macrovascular complications,e no. (%) 897 (28.2) 2283 (71.8) 10.3 (8.04) 9.34 (2.34) 635 (27.4) 119 (5.1)
to better treatment adherence. In fact, despite the high cost of SMBG, most patients in our sample had inadequate metabolic control, as found in previous studies.11,18 Factors other than effective SMBG are known to influence metabolic control, but it is clear that access to a HbA1c, glycated haemoglobin; NISS, National Institute of Social Security; SD, standard deviation.
a Afro-Brazilians, Mulattos, Asians, native Indians. b Data missing for 87 participants. c Includes preschool children, homemakers, volunteers and those who retired for reasons unrelated to
diabetes.
given technology does not guarantee its correct use by the patient or good adher- ence to recommendations. Continued education is helpful but depends on the d Defined as the time elapsed since diagnosis. e Excludes patients without criteria for the screening for diabetic complications (n = 863).
availability of capable staff trained for this purpose.
In a study of the costs associated costs calculated in this study are higher
with diabetes in Latin America, ap- than the costs found in studies that have
proximately US$ 607 were spent per mostly7 or exclusively included T2DM
patient annually, on average, in Chile patients,13 who use insulin far less often
and Mexico, whose gross national prod- than patients with T1DM. In 2007 in the
ucts are roughly equal to that of Brazil.7 United States, young insulin-treated pa-
In this study, however, cost estimates tients in the private health-care system
were based on a standard generalized faced costs that were 1.64 times higher
protocol that included three visits to than those faced by patients who were
a general practitioner, one visit to an not treated with insulin. The expendi-
ophthalmologist, one HbA1c test, one ture on diabetes supplies was 10 times
lipid profile, one electrocardiogram, higher among insulin-treated patients
one urine test (for proteinuria), and than among patients not treated with
treatment with insulin or oral drugs. insulin. Regardless of the treatment
Thus, the results do not reflect actual modality, outpatient expenditures con-
individualized clinical expenditures, and stituted the largest total expenditure (43
costs may have been underestimated. In and 58% for insulin-treated and non-
Brazil, the direct costs per capita and the insulin-treated youths with diabetes,
overall health expenditure associated
| 436
Bull World Health Organ 2013;91:434–440
doi: http://dx.doi.org/10.2471/BLT.12.110387
Bull World Health Organ 2013;91:434–440
Research Roberta Arnoldi Cobas et al. The cost of type 1 diabetes in Brazil Table 2. Average annual direct medical costs of inpatient and outpatient treatment of
type 1 diabetes mellitus, Brazil, 2008–2010
Average annual cost (US$)
with diabetes per capita were US$ 872 and US$ 270, respectively.7
In Brazil, the costs of certain drugs for diabetes and hypertension are fully
Popular Pharmacy Programme), devel- oped by the health ministry. The public system also provides SMBG supplies, Percentage of
Average
but not always in the amount needed or total cost
annual cost
recommended for optimal patient moni- per capita (US$)
toring and seldom uniformly across cit- Consultations 81 473.67 1.94 Tests 161 817.64 3.86 Outpatient treatment 3 867 915.66 92.20 Insulin 1 093 215.69 26.06 Oral drugs 87 782.17 2.09 Supplies for self–monitoring of blood glucose
25.62 50.89 1216.33 343.78 27.60
ies. Moreover, because the medications available through this programme do not always meet the patient’s needs, some treatment costs must be paid by the patient or his family. Therefore, diabetes drugs and supplies can take up a substantial fraction of a family’s income. Given that in 2009 the average Brazilian household had 3.1 members (4.2 if in the poorest socioeconomic category), any increase in household expenditures could undermine a fam- ily’s quality of life.19 Approximately 68% of the participants in our study were of low or very low economic status. To save money, these individuals may use their supplies inappropriately (e.g. they may reuse disposable supplies, use lower doses of medication or perform SMBG less often than recommended by clini- cal diabetes monitoring and treatment guidelines). As our results showed, the costs associated with diabetes are greater among patients of higher economic status. For patients of very low and low economic status, costs are 65% and 39% lower than for patients of high economic status. This may be because people of a higher educational level may seek and adhere to more complex and expensive therapeutic regimens.
A study conducted in Israel in the 1990s projected the estimated costs of T1DM over a 35-year period.20 The re- sults indicated that early in the disease, basic treatment accounts for approxi- mately 70% of total expenditures. How- ever, in the later stages the costs associ- ated with the complications of diabetes increase substantially.20 In the present study, the per capita costs rose with the duration of the diabetes. Patients who had had diabetes longer than 15 years had costs about 56% higher than those who had had the disease for less than 5 years. It is reasonable to assume that disease-related expenditures will rise in future years since costs increase in pro- portion to the duration of the diabetes and the incidence of T1DM is increasing among younger age groups.3 To date, no national multicentre epidemiological studies on the prevalence or incidence of T1DM have been conducted and the actual and future impact of the disease 2 215 749.68 52.82 696.78
Insulin pump and supplies 230 631.80 5.50 72.53 Medical procedures/haemodialysis 240 536.32 5.73 75.64 Hospitalizations 83 685.41 2.00 26.32 Total direct medical costs 4 194 892.39 100.00 1319.15
US$, United States dollar.
Table 3. Direct medical costs associated with type 1 diabetes mellitus, by patients’
demographic characteristics, Brazil, 2008–2010
Characteristic Mean (95% CI) direct medical cost
(US$)
P-value
Sex 0.294 Male 1288.23 (1 214.20–1362.25) Female 1343.13 (1 273.41–1412.85) Ethnicity 0.013 Caucasian 1374.85 (1 309.26–1440.43) Non-Caucasiana 1244.23 (1 164.07–1324.39) Age (years) 0.223 0–4 1145.00 (914.59–1375.41) 5–9 1047.83 (963.31–1132.36) 10–14 1198.92 (1 127.20–1270.64) 15–29 1306.83 (1 233.62–1380.03) ≥ 30 1564.72 (1 420.11–1709.34) Diabetes durationb (years) 0.000c < 5 1086.89 (1 023.51–1150.28) ≥ 5 but < 10 1220.69 (1 146.55–1294.82) ≥ 10 but < 15 1301.80 (1 194.11–1409.50) ≥ 15 1696.60 (1 549.52–1843.68) Socioeconomic status 0.000d High 1806.44 (1 565.34–2047.55) Medium 1561.45 (1 437.53–1685.37) Low 1302.24 (1 219.04–1385.45) Very low 1098.12 (1 022.02–1174.23)
CI, confidence interval; US$, United States dollar.
a Afro-Brazilians, Mulattos, Asians, native Indians. b Defined as the time elapsed since diagnosis. c P-value is for the following age comparisons: ≥ 15 years versus < 5 years; ≥ 15 years versus ≥ 5 but < 10
years; ≥ 15 years versus ≥ 10 but < 15 years. Other comparisons were not statistically significant. d P-value is for the following comparisons of socioeconomic status: high versus low; high versus very
low; medium versus low; medium versus very low. The comparison between high and medium socioeconomic status was not statistically significant.
subsidized by the public sector; the fed- eral government co-subsidizes private sector expenses through the Programa Farmácia Popular do Brasil (Brazilian
|
doi: http://dx.doi.org/10.2471/BLT.12.110387 437

Research The cost of type 1 diabetes in Brazil Roberta Arnoldi Cobas et al.
on the health-care system remains un-
reduces the risk of microvascular and determined.
macrovascular complications.2 Clinical Evaluating the costs associated with
and economic trials can furnish data diabetes becomes increasingly impor-
that can guide economic policy deci- tant in light of the expected increase
sions aiming to reduce direct costs in the prevalence of the disease and
by reallocating resources towards the its complications. In the present study,
prevention of acute and chronic com- the costs of type 1 diabetes increased
plications. in proportion to the duration of the
To our knowledge, this study is the diabetes. This increase may have an
first one in Latin America to estimate impact on health spending in the future
the costs associated with T1DM using because chronic complications become
data obtained from medical records. It more prevalent as diabetes progresses.
is representative of the distribution of In a Canadian study,21 the impact of
T1DM in Brazil and included different diabetes was projected over a 16-year
ethnic and socioeconomic groups from period. It found a projected increase in
all parts of the country. the number of diabetes patients from
Some limitations must be ad- 1.4 to 2.4 million and a projected 75%
dressed. The data used in this study were increase in health-care costs. However,
acquired from medical record reviews; the expected prevalence of diabetes and
thus, if any data were missing from the the costs associated with the disease
records, a data collection bias would increased in parallel with the ageing of
have led to an underestimation of the the population; the overall health-care
costs. Also, comparisons with studies costs for the youngest members of the
conducted in other countries are ham- population are not expected to increase
pered by the use of different currencies. substantially. Despite this projection,
Indeed, inflation and exchange rate dif- data from the Centers for Disease Con-
ferences may account for some of the trol and Prevention in Atlanta, United
discrepancies. Furthermore, the real States, indicate that annual health-care
costs of hospitalization for hypergly- costs among youths with diabetes are six
caemia or diabetic ketoacidosis exceed times higher than among youths without
the amount paid by the NBHCS, which diabetes.22
probably reimburses little more than Intervention studies, such as the
the costs of medications and laboratory DCCT, have shown that intensive treat-
tests and excludes daily hospital stay and ment during the early stages of T1DM
staff labour costs (data not shown). This,
صخلم ليزابرلا في ينطولا ديعصلا لىع زكارلما ةددعتم ةسارد :لولأا طمنلا نم يركسلا ءاد ةفلكت طمنلا نم يركسلا ءادل ةشرابلما ةيبطلا فيلاكتلا ديدتح ضرغلا ليزابرلا في ةيحصلا ةياعرلل ينطولا ماظنلل )T1DM( لولأا ةيلاجملإا ةفلكتلا في نوكم لك ماهسإ ةيعون ديدتحو )NBHCS( .يدرف وحن لىع لىع تاعاطقلا ةددعتم ةيعاجترسا ةسارد ءارجإ مت ةقيرطلا ةدايع 28 في 2010 لىإ 2008 نم ةترفلا في ينطولا ديعصلا 3180 لىع ةساردلا تلمتشاو .ةيليزارب ةنيدم 20 في ةيمومع ةنس 22 رمعلا طسوتم( لولأا طمنلا نم يركسلا ءادب اضيرم مهيقلت دنع ةيئاصقتسلاا ةسرادلل مهعاضخإ مت ثيح )11.8 ± .ليزابرلا في ةيحصلا ةياعرلل ينطولا ماظنلا نم ةيحصلا ةياعرلا متو .)8.0 ±( ةنس 10.3 ميهدل يركسلا ءاد ةدم طسوتم ناكو تاخضمو ةيبطلا تاءارجلإاو تارابتخلاا فيلاكت لىع لوصلحا ربلإاو نقاحلماو تادادملإاو ءاودلا لوانت تادادمإو ينلوسنلأا )SMBG( مدلا في زوكولغلا ىوتسلم تياذلا دصرلا لجأ نم لىإ 2010 نم ةترفلل ليحلماو ينطولا ةحصلا ماظن رداصم نم ةفاضإب ةشرابلما ةيونسلا ةيبطلا فيلاكتلا صلاختسا متو .2011 ةيبطلا تاراشتسلااو تارابتخلااو تادادملإاو ةيودلأا فيلاكت plus the fact that reimbursement by the NBHCS for medical and non-medical visits and procedures is low, could have led to an underestimation of the direct medical costs associated with diabe- tes from the perspective of the public health-care system in Brazil.
In conclusion, T1DM has an im- portant economic and social impact on the health-care system in Brazil. The direct costs associated with the disease are high, especially those as- sociated with drug treatment and sup- plies for insulin administration and SMBG. These findings should encour- age a reassessment of the distribution of resources for managing T1DM and trigger cost-effectiveness studies to optimize the long-term treatment of T1DM in Brazil. ■
Acknowledgements We thank Aline Kano and Elisangela Santos for their technical assistance.
Funding: This work was supported by grants from Farmanguinhos/Fundação Oswaldo Cruz/National Health Ministry, Brazilian Diabetes Society, Fundação do Amparo à Pesquisa do Estado do Rio de Janeiro and the Conselho Nacional de Desenvolvimento Científico e Tec- nológico do Brasil.
Competing interests: None declared.
ماعلا رادم لىع تايفشتسلما لىإ لوخدلا تارمو تاءار�جلإاو .ةلباقملل قباسلا 1319.15 درفلل ةشرابلما ةيونسلا ةيبطلا ةفلكتلا طسوتم غلب جئاتنلا 1216.33 – جلاعلاب لصتلما قافنلإا لثمو .ايكيرمأ ارلاود فيلاكتلا لياجمإ نم % 92.20 – ايونس ضيرملل ايكيرمأ ارلاود لىإ فيلاكتلا هذه لياجمإ نم % 52.82 ةبسن ىزعتو .ةشرابلما ةيبطلا زوكولغلا ىوتسلم تياذلا دصرلاو ينلوسنلأا لوانت ةرادإ تادادمإ ةبسن ىزعتو .)ايونس ضيرملل ايكيرمأ ارلاود 696.78( مدلا في ايكيرمأ ارلاود 75.64( ةشرابلما ةيبطلا فيلاكتلا نم % 5.73 ىزعتو .اعم مدلا لسغو ةيبطلا تاءارجلإا لىإ )ايونس ضيرملل ارلاود 25.62( ةشرابلما ةيبطلا فيلاكتلا نم % 1.94 ةبسن .تاراشتسلاا لىإ )ايونس ضيرملل ايكيرمأ نم يركسلا ءادل ةشرابم رثكلأا ةيبطلا فيلاكتلا ىزعت جاتنتسلاا دعاست نأ نكملما نمو .ةيحصلا تايجولونكتلا لىإ لولأا طمنلا يركسلا لىع ةرطيسلل دراولما عيزوت مييقت ةداعإ في تانايبلا هذه .ليزابرلا في ةيمومعلا ةيحصلا ةياعرلا ماظن في لولأا طمنلا نم
| 438
Bull World Health Organ 2013;91:434–440
doi: http://dx.doi.org/10.2471/BLT.12.110387
Bull World Health Organ 2013;91:434–440
Research Roberta Arnoldi Cobas et al. The cost of type 1 diabetes in Brazil 摘要 I 型糖尿病的成本 :巴西的全国多中心研究 目的 确定巴西国家医疗保健系统(NBHCS)I 型糖尿 病(T1DM)的直接医疗成本并量化每个组成部分对 总成本的贡献。 方法 2008 至 2010 年间,在巴西 20 个城市中的 28 个公立诊所执行全国范围内多中心的回顾式横断 面研究。研究纳入 3180 名 I 型糖尿病(平均年龄 22 ± 11.8 岁)患者,他们在接受 NBHCS 的医疗保 健过程中接受调查。糖尿病患者的平均患病期为 10.3 年(± 8.0)。从国家和地方卫生系统来源收集 2010- 2011 年的检测和医疗流程、胰岛素泵和用药、以及 自我血糖检测(SMBG)的耗材、注射器和针头的成本。 通过增加调查前一年的药物、耗材、检测、诊疗、流
程和住院的成本,推导年度直接医疗费用。 结果 人均平均年度直接医疗成本是 1319.15 美元。 治疗相关费用(每年每个病人 1216.33 美元)占总直 接医疗成本的 92.20%。胰岛素用药和 SMBG(每年 每个病人 696.78 美元)占总成本的 52.82%。医疗 流程和血液透析合计占直接医疗成本的 5.73%(每年 每个病人 75.64 美元)。诊疗占直接医疗成本的 1.94% (每年每个病人 25.62 美元)。
结论 卫生技术占绝大多数的 T1DM 直接医疗成本。 这些数据可用于对资源分配作出重新评估,进行巴西 公共卫生保健系统的 I 型糖尿病管理。
Résumé Coût du diabète de type 1: une étude multicentrique à l’échelle nationale réalisée au Brésil Objectif Déterminer les coûts médicaux directs du diabète gras de type 1 (DT1) pour le système de santé national brésilien (SSNB) et quantifier la contribution de chaque composante individuelle au coût total. Méthodes Une étude rétrospective, transversale, multicentrique et à l’échelle nationale a été menée entre 2008 et 2010 dans 28 cliniques publiques de 20 villes brésiliennes. Cette étude incluait 3180 patients atteints de DT1 (moyenne d’âge de 22 ans ± 11,8) qui ont été interrogés alors qu’ils étaient pris en charge par le SSNB. En moyenne, ils étaient atteints par la maladie depuis 10,3 ans (± 8). Les coûts des tests et des interventions médicales, des pompes à insuline et des équipements pour son administration, ainsi que des fournitures pour l’autosurveillance du taux de glycémie (ASTG) ont été obtenus à partir de sources provenant du système de santé national et local sur 2010–2011. Les coûts médicaux directs annuels ont été calculés en ajoutant les coûts des médicaments, des fournitures, des consultations médicales, des interventions et des
hospitalisations au cours de l’année précédant l’enquête. Résultats La moyenne du coût médical direct annuel par habitant s’élevait à 1319,15 dollars. Les dépenses liées au traitement – 1216,33 dollars par patient et par an –ont représenté 92,20% du total des coûts médicaux directs. L’équipement nécessaire à l’administration d’insuline et à l’ASTG (696,78 dollars par patient et par an) a totalisé 52,82% du total de ces coûts. Dans l’ensemble, les interventions médicales et l’hémodialyse ont représenté 5,73% (75,64 dollars par patient et par an) des coûts médicaux directs, et les consultations ont représenté 1,94% de ces mêmes coûts (25,62 dollars par patient et par an). Conclusion Les technologies de la santé ont constitué la majeure partie des coûts médicaux directs du DT1. Ces données peuvent être utilisées pour réévaluer la distribution des ressources pour la prise en charge du DT1 par le système de santé publique brésilien.
Резюме Расходы на лечение сахарного диабета 1-го типа: национальное многоцентровое исследование в Бразилии Цель Определить уровень прямых медицинских расходов, связанных с сахарным диабетом 1-го типа (T1DM), в Национальной системе здравоохранения Бразилии (NBHCS) и количественно определить долю каждого отдельного компонента в общей сумме расходов. Методы В 2008-2010 гг. было проведено ретроспективное, перекрестное, национальное многоцентровое исследование в 28 государственных клиниках в 20 городах Бразилии. В исследовании участвовало 3180 пациентов с T1DM (средний возраст: 22 года ± 11,8), опрошенных во время прохождения лечения в Национальной системе здравоохранения Бразилии. Средняя продолжительность заболевания диабетом у этих пациентов составляла 10,3 лет (± 8,0). Данные по стоимости тестов и медицинских процедур, дозаторов инсулина и расходных материалов, а также материалов, шприцев и игл для самостоятельного контроля уровня глюкозы в крови (SMBG) были получены из национальных и местных источников системы здравоохранения в течение 2010-2011 гг. Ежегодные прямые медицинские расходы рассчитывались методом сложения стоимости медикаментов, расходных материалов, тестов,
медицинских консультаций, процедур и госпитализации за год, предшествующий опросу. Результаты Среднегодовые прямые медицинские расходы на душу населения составили 1319,15 долларов США. Затраты на лечение – 1216,33 долларов США на пациента в год – составили 92,20% от общих прямых медицинских расходов. На самостоятельный контроль уровня глюкозы в крови и расходные материалы для ввода инсулина (696,78 долларов США на пациента в год) приходилось 52,82% от этой общей суммы расходов. Медицинские процедуры и гемодиализ в совокупности составили 5,73% (75,64 долларов США на пациента в год) от прямых медицинских расходов. На консультации приходилось 1,94% прямых медицинских расходов (25,62 долларов США на пациента в год). Вывод Основная доля прямых медицинских расходов на лечение T1DM приходилась на медицинские технологии. Эти данные могут способствовать пересмотру распределения ресурсов для лечения T1DM в государственной системе здравоохранения Бразилии.
|
doi: http://dx.doi.org/10.2471/BLT.12.110387 439

Research The cost of type 1 diabetes in Brazil Roberta Arnoldi Cobas et al.
Resumen El coste de la diabetes tipo 1: un estudio multicéntrico a nivel nacional en Brasil Objetivo Determinar los costes médicos directos de la diabetes mellitus de tipo 1 (DMT1) para el sistema nacional brasileño de atención sanitaria (NBHCS, según sus siglas en inglés) y cuantificar la contribución de cada componente individual al coste total. Métodos Se llevó a cabo un estudio multicéntrico retrospectivo transversal a nivel nacional entre los años 2008 y 2010 en 28 clínicas públicas de 20 ciudades brasileñas. El estudio incluyó 3180 pacientes con DMT1 (edad media de 22 años ± 11,8), que fueron entrevistados mientras recibían atención sanitaria del NBHCS. La duración media de su diabetes fue de 10,3 años (± 8,0). Los costes de las pruebas y procedimientos médicos, las bombas de insulina y provisiones para la administración, así como suministros para la automonitorización de la glucosa en sangre (AMG) se obtuvieron de las fuentes de los sistemas de salud nacionales y locales para el periodo 2010-2011. Los costes médicos directos anuales se obtuvieron sumando los costes de
los medicamentos, suministros, pruebas, consultas y procedimientos médicos y hospitalizaciones durante el año anterior a la entrevista. Resultados El coste medio directo anual por cápita fue de 1319,15 dólares americanos (US$). Los gastos relacionados con el tratamiento, US$ 1216,33 por paciente y año, representaron el 92,20% del total de los costes médicos directos. Los suministros para la administración de insulina y la AMG (US$ 696,78 por paciente y año) significaron el 52,82% de esos costes totales. En conjunto, los procedimientos médicos y la hemodiálisis representaron el 5,73% (US$ 75,64 por paciente y año) de los costes médicos directos. Las consultas fueron el 1,94% de los costes médicos directos (US$ 25,62 por paciente y año). Conclusión Las tecnologías sanitarias representaron la mayoría de los costes médicos directos de la DMT1. Estos datos pueden servir para volver a examinar la distribución de los recursos para la gestión de la diabetes de tipo 1 en el sistema de salud pública de Brasil.
References 1. American Diabetes Association. Standards of medical care in
diabetes–2012. Diabetes Care 2012;35(Suppl 1):S11–63. doi: http://dx.doi. org/10.2337/dc12-s011 PMID:22187469 2. The Diabetes Control and Complications Trial Research Group. The
effect of intensivetreatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med 1993;329:977–86. doi: http://dx.doi.org/10.1056/ NEJM199309303291401 PMID:8366922 3. DIAMOND Project Group. Incidence and trends of childhood Type 1
diabetes worldwide 1990–1999. Diabet Med 2006;23:857–66. PMID:16911623 4. Ferreira SR, Franco LJ, Vivolo MA, Negrato CA, Simoes AC, Ventureli CR. Population-based incidence of IDDM in the state of São Paulo, Brazil. Diabetes Care 1993;16:701–4. doi: http://dx.doi.org/10.2337/ diacare.16.5.701 PMID:8495607 5. Negrato CA, Dias JP, Teixeira MF, Dias A, Salgado MH, Lauris JR et al.
Temporal trends in incidence of Type 1 diabetes between 1986 and 2006 in Brazil. J Endocrinol Invest 2010;33:373–7. PMID:19620822 6. Laing SP, Swerdlow AJ, Slater SD, Burden AC, Morris A, Waugh NR
et al. Mortality from heart disease in a cohort of 23,000 patients with insulin-treated diabetes. Diabetologia 2003;46:760–5. doi: http://dx.doi. org/10.1007/s00125-003-1116-6 PMID:12774166 7. Barceló A, Aedo C, Rajpathak S, Robles S. The cost of diabetes in Latin
America and the Caribbean. Bull World Health Organ 2003;81:19–27. PMID:12640472 8. American Diabetes Association. Economic costs of diabetes in the US in
2007. Diabetes Care 2008;31:596–615. doi: http://dx.doi.org/10.2337/dc08- 9017 PMID:18308683 PMID:18308683 9. Nathan DM, Cleary PA, Backlund JY, Genuth SM, Lachin JM, Orchard TJ
et al.; Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications (DCCT/EDIC) Study Research Group. Intensive diabetes treatment and cardiovascular disease in patients with type 1 diabetes. N Engl J Med 2005;353:2643–53. doi: http://dx.doi. org/10.1056/NEJMoa052187 PMID:16371630 10. The Diabetes Control and Complications Trial Research Group. Lifetime
benefits and costs of intensive therapy as practiced in the diabetes control and complications trial. JAMA 1996;276:1409–15. doi: http://dx.doi. org/10.1001/jama.1996.03540170053032 PMID:8892716 11. Gomes MB, Coral M, Cobas RA, Dib SA, Canani LH, Nery M et al. Prevalence
of adults with type 1 diabetes who meet the goals of care in daily clinical practice: a nationwide multicenter study in Brazil. Diabetes Res Clin Pract 2012;97:63–70. doi: http://dx.doi.org/10.1016/j.diabres.2012.02.008 PMID:22397904
12. Govan L, Wu O, Briggs A, Colhoun HM, McKnight JA, Morris AD et al.;
Scottish Diabetes Research Network Epidemiology Group. Inpatient costs for people with type 1 and type 2 diabetes in Scotland: a study from the Scottish Diabetes Research Network Epidemiology Group. Diabetologia 2011;54:2000–8. doi: http://dx.doi.org/10.1007/s00125-011-2176-7 PMID:21607632 13. González JC, Walker JH, Einarson TR. Cost-of-illness study of type 2 diabetes
mellitus in Colombia. Rev Panam Salud Publica 2009;26:55–63. doi: http:// dx.doi.org/10.1590/S1020-49892009000700009 PMID:19814883 14. Bahia LR, Araújo DV, Schaan BD, Dib SA, Negrato CA, Leão MPS et al. The
costs of type 2 diabetes mellitus outpatient care in the Brazilian public health system. Value Health 2011;14(Suppl 1):S137–40. doi: http://dx.doi. org/10.1016/j.jval.2011.05.009 PMID:21839888 15. Associação Brasileira de Empresas de Pesquisa [Internet]. Critério de
classificação econômica Brasil (CCEB) - em vigor a partir de 01/02/2012. São Paulo: ABEP; 2013. Portuguese. Available from: http://www.abep.org/novo/ Content.aspx?SectionID=84 [accessed 30 March 2013]. 16. Sistema Único de Saúde [Internet]. Portal da saúde, banco de preços em saúde. SUS; 2013. Portuguese. Available from: http://portal.saude.gov.br/ portal/saude/Gestor/area.cfm?id_area=939 [accessed 30 March 2013]. 17. Shrestha SS, Zhang P, Albright A, Imperatore G. Medical expenditures
associated with diabetes among privately insured US youth in 2007. Diabetes Care 2011;34:1097–101. doi: http://dx.doi.org/10.2337/dc10-2177 PMID:21525502 18. Gomes MB, de Mattos Matheus AS, Calliari LE, Luescher JL, Manna TD,
Savoldelli RD et al. Economic status and clinical care in young type 1 diabetes patients: a nationwide multicenter study in Brazil. Acta Diabetol 2012. Epub 12 June. PMID:22688518 19. Instituto Brasileiro de Geografia e Estatística [Internet]. Uma análise das
condições de vida da população brasileira 2010. Rio de Janeiro: IBGE; 2013. Portuguese. Available from: http://www.ibge.gov.br/home/estatistica/ populacao/condicaodevida/indicadoresminimos/sinteseindicsociais2010/ default.shtm [accessed 30 March 2013]. 20. Stern Z, Levy R. The direct cost of type 1 diabetes mellitus in Israel. Diabet
Med 1994;11:528–33. doi: http://dx.doi.org/10.1111/j.1464-5491.1994. tb02031.x PMID:7955968 21. Ohinmaa A, Jacobs P, Simpson S, Johnson JA. The projection of prevalence
and costs of diabetes in Canada: 2000 to 2016. Canadian J Diabetes 2004;28:1–8. 22. Centers for Disease Control and Prevention [Internet]. Diabetes public
health resource. Atlanta: CDC; 2012. Available from: http://www.cdc.gov/ diabetes/ [accessed 30 March 2013].
| 440
Bull World Health Organ 2013;91:434–440
doi: http://dx.doi.org/10.2471/BLT.12.110387

Copyright of Bulletin of the World Health Organization is the property of World Health Organization and its content may not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's express written permission. However, users may print, download, or email articles for individual use.